Download
1 / 1
20 likes | 194 Views
What is competence?. E. Conclusion. Introduction. Method. E. What are the barriers to achieving it?. What is Competence? Trainees’ perception of achieving competence in Obstetrics and Gynaecology Modarres M 1, 2 , Chase AR 1 , Chappatte OA 1 , Flint S 1,2

E N D
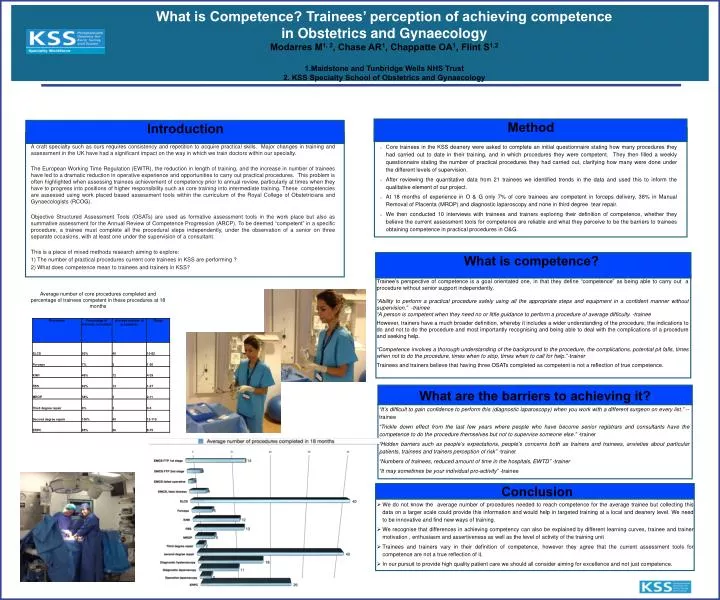
What is competence? E Conclusion Introduction Method E What are the barriers to achieving it? What is Competence? Trainees’ perception of achieving competence in Obstetrics and Gynaecology Modarres M1, 2, Chase AR1, Chappatte OA1, Flint S1,2 1.Maidstone and Tunbridge Wells NHS Trust 2. KSS Specialty School of Obstetrics and Gynaecology Learner Characteristics A craft specialty such as ours requires consistency and repetition to acquire practical skills. Major changes in training and assessment in the UK have had a significant impact on the way in which we train doctors within our specialty. The European Working Time Regulation (EWTR), the reduction in length of training, and the increase in number of trainees have led to a dramatic reduction in operative experience and opportunities to carry out practical procedures. This problem is often highlighted when assessing trainees achievement of competency prior to annual review, particularly at times when they have to progress into positions of higher responsibility such as core training into intermediate training. These competencies are assessed using work placed based assessment tools within the curriculum of the Royal College of Obstetricians and Gynaecologists (RCOG). Objective Structured Assessment Tools (OSATs) are used as formative assessment tools in the work place but also as summative assessment for the Annual Review of Competence Progression (ARCP). To be deemed “competent” in a specific procedure, a trainee must complete all the procedural steps independently, under the observation of a senior on three separate occasions, with at least one under the supervision of a consultant. This is a piece of mixed methods research aiming to explore: 1) The number of practical procedures current core trainees in KSS are performing ? 2) What does competence mean to trainees and trainers in KSS? • Core trainees in the KSS deanery were asked to complete an initial questionnaire stating how many procedures they had carried out to date in their training, and in which procedures they were competent. They then filled a weekly questionnaire stating the number of practical procedures they had carried out, clarifying how many were done under the different levels of supervision. • After reviewing the quantitative data from 21 trainees we identified trends in the data and used this to inform the qualitative element of our project. • At 18 months of experience in O & G only 7% of core trainees are competent in forceps delivery, 38% in Manual Removal of Placenta (MROP) and diagnostic laparoscopy and none in third degree tear repair. • We then conducted 10 interviews with trainees and trainers exploring their definition of competence, whether they believe the current assessment tools for competence are reliable and what they perceive to be the barriers to trainees obtaining competence in practical procedures in O&G. Trainee’s perspective of competence is a goal orientated one, in that they define “competence” as being able to carry out a procedure without senior support independently. “Ability to perform a practical procedure safely using all the appropriate steps and equipment in a confident manner without supervision.” -trainee “A person is competent when they need no or little guidance to perform a procedure of average difficulty. -trainee However, trainers have a much broader definition, whereby it includes a wider understanding of the procedure, the indications to do and not to do the procedure and most importantly recognising and being able to deal with the complications of a procedure and seeking help. “Competence involves a thorough understanding of the background to the procedure, the complications, potential pit falls, times when not to do the procedure, times when to stop, times when to call for help.”-trainer Trainees and trainers believe that having three OSATs completed as competent is not a reflection of true competence. Average number of core procedures completed and percentage of trainees competent in these procedures at 18 months “It’s difficult to gain confidence to perform this (diagnostic laparoscopy) when you work with a different surgeon on every list.” --trainee “Trickle down effect from the last few years where people who have become senior registrars and consultants have the competence to do the procedure themselves but not to supervise someone else.” -trainer “Hidden barriers such as people’s expectations, people’s concerns both as trainers and trainees, anxieties about particular patients, trainees and trainers perception of risk” -trainer “Numbers of trainees, reduced amount of time in the hospitals, EWTD” -trainer “It may sometimes be your individual pro-activity” -trainee • We do not know the average number of procedures needed to reach competence for the average trainee but collecting this data on a larger scale could provide this information and would help in targeted training at a local and deanery level. We need to be innovative and find new ways of training. • We recognise that differences in achieving competency can also be explained by different learning curves, trainee and trainer motivation , enthusiasm and assertiveness as well as the level of activity of the training unit • Trainees and trainers vary in their definition of competence, however they agree that the current assessment tools for competence are not a true reflection of it. • In our pursuit to provide high quality patient care we should all consider aiming for excellence and not just competence.