Download
1 / 14
180 likes | 544 Views
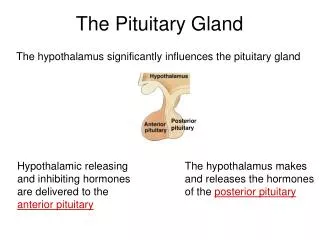
Pituitary Gland Disorders. Omar DHAIMAT MD. Introduction. Six hormones are secreted by the anterior pituitary gland:ACTH,TSH,LH,FSH,GH,PrL. Two hormones are secreted by the posterior part:ADH,Oxytocin. Understand hypopituitarism. Pituitary tumors. Hypopituitarism.

E N D
Pituitary Gland Disorders Omar DHAIMAT MD
Introduction • Six hormones are secreted by the anterior pituitary gland:ACTH,TSH,LH,FSH,GH,PrL. • Two hormones are secreted by the posterior part:ADH,Oxytocin. • Understand hypopituitarism. • Pituitary tumors.
Hypopituitarism • Causes of hypopituitarism(hypothalamic versus pituitary). • Either will result in deficiency of the hormones: (hypothyroidism ,hypogonadism, adrenal insufficiency,postpartum lactation failure,short stature).
Diagnosis: • Low serum levels of the appropriate pituitary hormone concurrent with low levels of the target –organ hormone. • Stimulation tests: • 1.GH: insulin,Arginine,l-dopa with or without propranalol.
Diagnosis: • 2. PrL: TRH,Metoclopramide. • 3.TSH: TRH. • 4.LH&FSH: GnRH,Clomiphene. • 5.ACTH: insulin,Metyrapone,Cosyntropin.
Treatment: • Give the deficient end organ hormones. • Pituitary hormone replacement:growth hormone,HCG(for LH). • Bracelet identification.
Apoplexy .Means loss of consciousness followed by paralysis. Classic pit.apo is an acute life threatening event characterized by severe headache and collapse with evidence of pituitary hemorrhage. Cranial nerves affected:2,3,4,6 ,7. Associated with hypopit.No post. Sub acute forms(dm,Scell).
Pituitary Tumors: • 10% of brain tumors. • Benign. • Most common:PrL(26%),Nonfun(23%), • Least common: TSH(1%). • S&S related to mass effect,and excessive hormone production. • Macro adenoma (>1cm).
Acromegaly&gigantism • Features: gigantism:increased stature,before closure of epiphysis.Sweating,CTS,arthritis,hypertension,dm,Hypercalciuria,galactorrhea,sleep apnea,colon polyps.Enlargement of facial features,hands and feet. • DX: most sensitive IGF1 are elevated.No suppression to O.Glucose.Base line PrL can be high due to mixed tumors.Imaging study: MRI,CT.Visual field examination.
Acromegaly&gigantism • Treatment :surgery(TSS) then radiotherapy or Octreotide.Bromocriptine can be used with less effect. • Cure: 1.Fasting growth hormone<5ng/ml.2.GH level<1 ng/ml following oral glucose.3.Normal level of IGF1.
Prolactinoma: • Most common. • Features: women(amenorrhea,with or without galactorrhea).Men(decreased libido&potency).Also,mass effect.
Prolactinoma: • Dx :exclude pregnancy,hypothyrodism and renal failure.Persistent PrL >200ng/ml.Stimulation test: TRH ,show no response. • Treatment:dopamine agonist(Bromocriptine,Lisuride,pergolide and CABERGOLINE).Surgery &RT are second line.
Pituitary Tumors • TSH secreting tumors:rare,Hyperthyroidism features with goiter,high TSH,T4,T3 AND HIGH ALPHA SUBUNIT.No response to TRH.
Pituitary Tumors • Treatment: surgery or RT. • Gonadotropin-secreting tumors:are responsible for most non functioning tumors.FSH,LH AND alpha or beta subunit.Macro adenomas:headaches,visual changes and occasionally hypopituitarism.Testicular enlargement in men with FSH tumors.Treatment:surgery with RT.