Download
1 / 11
120 likes | 246 Views
SPSP Fellowship Project Charter. To create, implement and maintain a medicines reconciliation process in an outpatient Pain Clinic David Hill. What are we trying to accomplish ? (context and problem). NPSA “Safety in Doses” Medication errors common Local problems:

E N D
SPSP Fellowship Project Charter To create, implement and maintain a medicines reconciliation process in an outpatient Pain Clinic David Hill
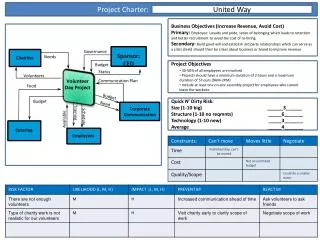
What are we trying to accomplish ?(context and problem) • NPSA “Safety in Doses” • Medication errors common • Local problems: • Wasted clinic time trying to achieve accurate meds • Had to book repeat visits • Patients phone confused about changes • GP’s phone confused about changes • Have allowed harm by not recognising hazardous medication
What are we trying to accomplish ?(benefits of improvement) • Ensure every consultation based on medications patient actually taking • Successfully communicate changes to: • Patient • GP • Ensure interventions are only carried out when: • Patient not taking anticoagulants • Patient not on antibiotics • All allergies identified
What are we trying to accomplish ?(Aims) • To accurately & completely reconcile medications in at least 95% of Chronic Pain Clinic patients by September 2010 • To identify hazardous medication & allergies in 100% of patients by September 2010
What are we trying to accomplish (Goals) • Engage clinical team & reach agreement to improve • by end of December 2009 • Collect some baseline data • by end of Jan 2010 • Test initial changes • by end of Feb 2010 • Reconcile medications in 95% • by Sept 2010 • Identify anticoagulants/antibiotics/allergies in 100% • by Sept 2010 • Compensate for extra consultation time • by Dec 2010
How will we know that change is an improvement? • Measurement plan- • 20 charts/patients a month • By DH & CF • Data loaded onto Trust “extranet” • Analysis • Annotated monthly run charts and graphs • Financial impact • Cost of forms & secretary time • Prevention of revisits
What changes can we make that will result in improvement? • Initial activities • Form team • Collect baseline data • Convene focus group • Process map flow of medication information • Create ideas to achieve goals • Discuss adapting changes from other settings • Review available literature & discuss
What changes can we make that will result in improvement? Initial PDSA cycles • Test letter to get patient to bring meds • Test Meds Rec Form (MRF) • Test checklist to detect hazardous meds • Test communication to GP
Participation Improvement Team • Improvement advisor: NoeleenDevaney • Sponsor: Charlie Martyn (MD) • Process owner: Bob Darling (CD) • Team Leader: David Hill • Team members: • Conor Farrell (Pain Fellow) • Kerry Wade (CNS) • Karen Armstrong (secretary) • Neville McMullan (GP) • Erika Hughes (pharmacist) • Patient?