Download
1 / 1
30 likes | 200 Views
Hypoxia Training in the U.S. Navy – A New Instructional Paradigm – A.R. Artino, W.L. Collins, T.P. Sudduth, B.D. Swan, M.C. Prevost, H.L. Phillips Naval Operational Medicine Institute, Naval Survival Training Institute, Pensacola, Florida. INTRODUCTION

E N D
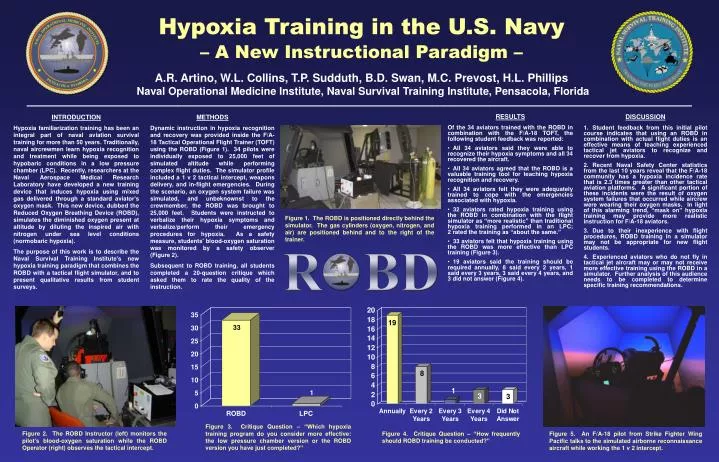
Hypoxia Training in the U.S. Navy– A New Instructional Paradigm – A.R. Artino, W.L. Collins, T.P. Sudduth, B.D. Swan, M.C. Prevost, H.L. PhillipsNaval Operational Medicine Institute, Naval Survival Training Institute, Pensacola, Florida INTRODUCTION Hypoxia familiarization training has been an integral part of naval aviation survival training for more than 50 years. Traditionally, naval aircrewmen learn hypoxia recognition and treatment while being exposed to hypobaric conditions in a low pressure chamber (LPC). Recently, researchers at the Naval Aerospace Medical Research Laboratory have developed a new training device that induces hypoxia using mixed gas delivered through a standard aviator's oxygen mask. This new device, dubbed the Reduced Oxygen Breathing Device (ROBD), simulates the diminished oxygen present at altitude by diluting the inspired air with nitrogen under sea level conditions (normobaric hypoxia). The purpose of this work is to describe the Naval Survival Training Institute's new hypoxia training paradigm that combines the ROBD with a tactical flight simulator, and to present qualitative results from student surveys. METHODS Dynamic instruction in hypoxia recognition and recovery was provided inside the F/A-18 Tactical Operational Flight Trainer (TOFT) using the ROBD (Figure 1). 34 pilots were individually exposed to 25,000 feet of simulated altitude while performing complex flight duties. The simulator profile included a 1 v 2 tactical intercept, weapons delivery, and in-flight emergencies. During the scenario, an oxygen system failure was simulated, and unbeknownst to the crewmember, the ROBD was brought to 25,000 feet. Students were instructed to verbalize their hypoxia symptoms and verbalize/perform their emergency procedures for hypoxia. As a safety measure, students' blood-oxygen saturation was monitored by a safety observer (Figure 2). Subsequent to ROBD training, all students completed a 20-question critique which asked them to rate the quality of the instruction. RESULTS Of the 34 aviators trained with the ROBD in combination with the F/A-18 TOFT, the following student feedback was reported: • All 34 aviators said they were able to recognize their hypoxia symptoms and all 34 recovered the aircraft. • All 34 aviators agreed that the ROBD is a valuable training tool for teaching hypoxia recognition and recovery. • All 34 aviators felt they were adequately trained to cope with the emergencies associated with hypoxia. • 32 aviators rated hypoxia training using the ROBD in combination with the flight simulator as “more realistic” than traditional hypoxia training performed in an LPC; 2 rated the training as “about the same.” • 33 aviators felt that hypoxia training using the ROBD was more effective than LPC training (Figure 3). • 19 aviators said the training should be required annually, 8 said every 2 years, 1 said every 3 years, 3 said every 4 years, and 3 did not answer (Figure 4). DISCUSSION • Student feedback from this initial pilot course indicates that using an ROBD in combination with actual flight duties is an effective means of teaching experienced tactical jet aviators to recognize and recover from hypoxia. • Recent Naval Safety Center statistics from the last 10 years reveal that the F/A-18 community has a hypoxia incidence rate that is 2.3 times greater than other tactical aviation platforms. A significant portion of these incidents were the result of oxygen system failures that occurred while aircrew were wearing their oxygen masks. In light of this alarming trend, “mask on” hypoxia training may provide more realistic instruction for F/A-18 aviators. • Due to their inexperience with flight procedures, ROBD training in a simulator may not be appropriate for new flight students. • Experienced aviators who do not fly in tactical jet aircraft may or may not receive more effective training using the ROBD in a simulator. Further analysis of this audience needs to be completed to determine specific training recommendations. Figure 1. The ROBD is positioned directly behind the simulator. The gas cylinders (oxygen, nitrogen, and air) are positioned behind and to the right of the trainer. Figure 3. Critique Question – “Which hypoxia training program do you consider more effective: the low pressure chamber version or the ROBD version you have just completed?” Figure 2. The ROBD Instructor (left) monitors the pilot's blood-oxygen saturation while the ROBD Operator (right) observes the tactical intercept. Figure 4. Critique Question – “How frequently should ROBD training be conducted?” Figure 5. An F/A-18 pilot from Strike Fighter Wing Pacific talks to the simulated airborne reconnaissance aircraft while working the 1 v 2 intercept.