Download
1 / 41
410 likes | 527 Views
to medicines The Access ^ Gap. Universities Allied for Essential Medicines University of Florida August 31, 2006 Thanks to UPenn & Berkeley. Key Global Diseases. AIDS Diabetes in Eastern Africa & India Heart disease in South & Southeast Asia Hepatitis in Eastern Europe & Russia

E N D
to medicines The Access ^ Gap Universities Allied for Essential Medicines University of Florida August 31, 2006 Thanks to UPenn & Berkeley
Key Global Diseases • AIDS • Diabetes in Eastern Africa & India • Heart disease in South & Southeast Asia • Hepatitis in Eastern Europe & Russia • Neglected diseases in Latin America and Africa
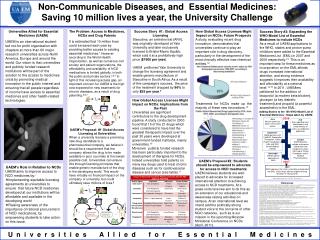
The Problem • 1/3 of the world lacks access to essential medicines1 • Essential Medicines are “those that satisfy the priority health care needs of the population”2 • “It is estimated that by improving access to existing essential medicines and vaccines, about 10 million lives per year could be saved.” 3 1. Medecins Sans Frontieres. http://www.accessmed-msf.org/campaign/faq.shtm 2. World Health Organization. http://www.who.int/medicines/services/essmedicines_def/en/ 3. World Health Organization. Equitable access to essential medicines: a framework for collective action. Geneva: 2004.
Terminology • LMIs: Low- and middle-income countries • World Bank designation based on gross national income (GNI) per capita • Low-income countries • E.g. Haiti, Rwanda, Vietnam • Middle-income countries • E.g. China, Brazil, Botswana • High-income countries • E.g. Japan, USA, Israel http://web.worldbank.org/WBSITE/EXTERNAL/DATASTATISTICS/0,,contentMDK:20421402~pagePK:64133150~piPK:64133175~theSitePK:239419,00.html
The World Market Source: IMS Health, 2002
Three Gaps to Access Pecoul, PLoS Med. 2004
What is a neglected disease? Yamey, Brit. Med. J. 2002 Molyneux et al., PLoS Med 2005
The landscape of R&D for neglected diseases • Push and pull incentives • Push: direct funding or facilitation of research and development (grants) • Pull: promise downstream rewards by organizing a market for eventual end products (patents) • Public-private partnerships (PPPs) • Virtual R&D management
Bridging the research gap • ND research exemptions • Univ. gives research data to nonprofits for use in researching NDs • ND research promotion • Incentives for researchers, Univ. marketing • Progressive technology transfer metrics • Money for university and impact on global human welfare
Public Domain Belongs to no one/ everyone Can be freely used for any purpose (make, use, sell, modify, build upon) Creates a “commons” of knowledge and culture from which everyone can draw Intellectual property Private rights create incentives to research, create, develop, and market products Gap 2: Development
Basics of a Patent • What you give: description of invention, explain how it works, disclose how to make it • What you get: set of exclusive rights for 20 years to prevent others from making, using, selling, offering to sell or importing a claimed invention • Since your patent expires in twenty years, it encourages you to make your invention widely available to extract maximum profit before it enters the public domain
“ What role do universities play?” • Universities’ role increasing as an important part U.S. R&D U.S. universities are responsible for more than 50% of the country’s basic research science • Growth in patenting and commercialization • 1970 to 2001, ten-fold increase in number of U.S. patents issued annually to U.S. academic institutions • AUTM data show significant increase in licensing activity • Major players in the biopharmaceutical arena 40%-50% of the drug industry’s new products rely heavily upon academic research
Increase in Patenting and Commercialization: Bayh-Dole Act (1980) • Goal: • Increase technology transfer and utilization of federally-funded research • What did it do? • Universities given right to retain the property rights to inventions made under federal funding; exclusive licensing permitted • Growth in Patenting • (faster than other patenting in the United States) • Surge in Licensing Activity • Increase in Royalties from Licensing
How this applies to UF • Bob is a researcher at UF • Bob invents a vaccine for AIDS • Bob (UF) patents his invention • Technically, Bob is working for UF • Therefore, Bob doesn’t own the patent, UF does • UF now has an exclusive right to AIDS vaccine which it licenses to the highest bidder for production
Conventional Pipeline University Patents IP Patent Drugpatents Licensing Agreement Exclusive Marketing Rights High-income countries LMI Countries
Pricing and Patents Why Focus on Pricing? • Pharmaceutical purchasing is large economic burden • Drugs comprise the largest share of household expenditures in developing countries World Health Organization. http://www.who.int/medicines/services/essmedicines_def/en/
Pricing and Patents • How do patents raise drug prices? • Patents grant temporary monopolies on drug sales • Without competition, no incentive for price reduction HMS, 2002
Pricing and Patents Why Focus on Pricing? • When drugs are cheaper, more people can use them • When people know that they can afford the treatment, they will get tested. • Rate of HIV testing rises when AIDS treatments are more available* *Castro A and Farmer P. Understanding and addressing AIDS-related stigma: from anthropological theory to clinical practice in Haiti. Am J Public Health. 2005 Jan;95(1):53-9.
Effects of Generics MSF 2003
The Equitable Access License(EAL) IP Patent Drug patents Exclusive Licensing Agreement Marketing High-income countries LMI Marketing Rights LMI Countries Generic Manufacturer(s) Marketing
The Equitable Access License (EAL) Why is it promising? • Simple • Requires no institutionalized oversight or enforcement • PR potential for Universities • Vast majority of pharmaceutical revenue unaffected • Only 5-7% revenue from LMIs* • All of Africa accounts for just over 1%** • No negative impact post-d4t *Pharmaceutical Research and Manufacturers of America. Pharmaceutical Industry Profile 2005 – From Laboratory to Patient: Pathways to Biopharmaceutical Innovation. Washington, DC: 2005 **Medicins Sans Frontieres. http://www.accessmed-msf.org/campaign/faq.shtm
Potential BENEFIT to UF • Possible financial benefits: small but significant revenue stream from its share of royalties for generic end products that would otherwise not be sold in poor countries • Combining access-oriented licensing policies with an augmented neglected-disease research agenda can help UF aggressively position itself as a research center for foundation-sponsored partnerships. • Intangible Benefits: UF can establish itself as a leader in defining the role universities can play in closing the global access gap.
The case of Berkeley • Berkeley’s Socially Responsible Licensing Initiative aims to: a) promote widespread availability of technology and healthcare in the developing world, b) share revenue with a contributor of the research and/or to give proper attribution to a source or collaborator, and c) stimulate additional investment by others to achieve these goals. • "In the new reality we can have a double bottom line, we can have the financial bottom line, and we can have the societal-impact bottom line.” Carol Mimura
Case StudyYale: the d4T story • In 2001, Yale students protested their university’s refusal to yield its patent rights to the HIV drug d4T, or Stavudine, in Africa. • In Africa, an estimated 25 million people are infected with the HIV virus. • This quickly snowballed into a battle over the place of university research in modern medicine. • D4T, was discovered by Yale pharmacology professor and licensed exclusively to drug giant Bristol-Myers Squibb Co. • Yale administrators argued Yale had already ceded its licensing rights to Bristol-Myers, but acted quickly to push the company to allow generic drug makers to sell low-cost versions of the drug
Implications For South Africa • Rapid, thirty-fold reduction in the price of d4t in South Africa (from more than $1600 to $55 per patient per year) • August 2003, Aspen began selling generic d4t in South Africa for up to 40% less than the reduced BMS price • The national ARV program being rolled out in South Africa will rely upon generic versions of d4t For Yale • No loss of income associated • Subsequent major Pfizer investment
Gap 3: Delivery per 100 000 pop < 10 10 - 24 25 - 49 50 - 99 100 - 299 300 or more No estimate Estimated TB Incidence Rates, 2001
Lingering Problems • Limited resources of humanitarian organizations • Generic motivation is still profit • Lack of existing infrastructure such as roads • Political climate • Other related problems such as food
UAEM Goals • Student body awareness of the access to medicines gap • Educate members about the issue and ways we can help through speakers and events • Encourage UF to look for proactive solutions the university can implement
Licensing difficulties of generic biologics; different federal regulatory paths Better World Project to increase innovation Lack of existing infrastructure and cultural barriers How to lower the price of R&D More at uaemuf.wordpress.com FL Tech Transfer Conference
Allies @ UF Mary Ann Burg, Ph.D., L.C.S.W. Director of UF’s Women’s Health Research Center Faculty Senate Member Robert Hatch, M.D., MPHAssociate Professor Department of Community Health and Family Medicine Danaya Wright, J.D., Ph.D.Law Professor Incoming Faculty Senate President Marta Wayne, Ph.D. Assistant professor of zoology
Get Involved! • Through classes – many have international/research focus • Through research – check out the undergraduate research database or browse faculty webpages • Through organizations – UAEM among a host of others
Upcoming Dates • Journal Club – September 14th Every 2nd Thursday following • Meeting – September 21st 1st and 3rd Thursdays of the month • Elections – November 30th http://uaemuf.wordpress.com/calendar/ See you there!