Download

1 / 48
480 likes | 608 Views
Ultrasonographic studies of the lower urinary Tract, Anorectal Tract and Pelvic Floor. p.bastani Tabriz university of medical science.

E N D
Ultrasonographic studies of the lower urinary Tract, Anorectal Tract and Pelvic Floor p.bastani Tabriz university of medical science
Two and Three-dimensional ultrasound imaging are gaining in popularity within the clinical setting and are sometimes replaced radiography in the evaluation of pelvic floor disorders,because of: ·non invasiveness ·reproducibility ·nonradiation exposure ·and less expense
Many approaches have been proposed for the evaluation of the lower urinary tract by urltrasound. These include transabdominal, transrectal, perineal (or translabial )and introital approachs.
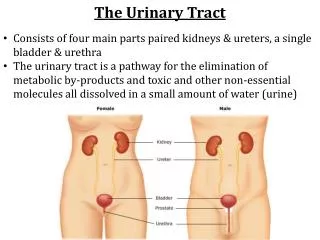
* The examination can be performed in dorsal lithotomy. Semi-recumbent or standing position. * The image must be oriented in the sagittal position to obtain accurate data from symphsis pubis,urethra,bladder neck, vagina, cervix,rectum and annual canal.
Ultrasound assessment of the Anterior Zone change in urethral diameter during straining may be used to assess the integrity of the urethral and bladder neck closure mechanisms. Bladder base descent greater than 10 mm and funnelling during straining might suggest a pubourethral (pul) defect. Repeating this manoeuvre after unilateral anchoring at midurethra restores geometry and continence (petros & von Konsky)
Ultrasound Assessment of the Middle Zone Knowledge of the Middle zone and its relationship to the anterior and Posterior zones can be obtained by observing changes in morphology During straining, coughing and after anchoring various connective structures.
Ultrasonography after surgery After anterior and middle zones defect repair with mesh, it can be accurately identified by Ultrasound
Ultrasound assessment of posterior zone Pointing the probe more posteriorly, one can resualize the anus, rectum, longitudinal muscle of the anus (LMA) and levator plate (lp)
The benefits are: * Endosonography allows visualization of defects in the internal and external sphincters. * Additionally the pictures obtained from endosonography provide a road map for repair of the sphincter.
Orientation of the probe in a female patient showingthe “U” sling of the puborectalis (PR) with vagina anterior
Complete division of the internal anal sphincterwith a defect (arrows) high in the canal at the level of thepuborectalis (PR)
benefits Also with endosonography we can follow anal fistula. If an external opening can be identified, some doctors will introduce hydrogen peroxide H2O2 (3-5%) in to opening immediately before acquiring a 2D or 3D data set. The H2O2 enhances the fistula tracts so that they appear bright with structures in the ultrasound image.
Anorectal ultrasonography *Endosonography is recognized as a valuable tool in the assessment of Anorectal problems. * An endoanal probe must permit a 360° image mode and it must facilitate a high center frequency. * The probe head diameter should be relatirely small and cylindrical for maneavering the transducer in the anal canal.
At last: Ultrasound is a relatively inexpensive office tool which allows the clinician to determine the dynamic geometry of pelvic organs at rest. During effort, to identify the pelvic muscles, their movement relative to rest, and the location of implanted tapes and meshes.