Download
1 / 20
210 likes | 415 Views
Objective Measurement for Lumbar Spinal Angels Submitted To Prof. Dr. Maher El-keblawy Professor of Basic Science Department Faculty of Physical Therapy Cairo University. The specific parts that make up the spine. 1. Vertebrae ( five vertebral bodies). 2. Intervertebral Disc.

E N D
Objective Measurement for Lumbar Spinal Angels Submitted To Prof. Dr. Maher El-keblawy Professor of Basic Science Department Faculty of Physical Therapy Cairo University
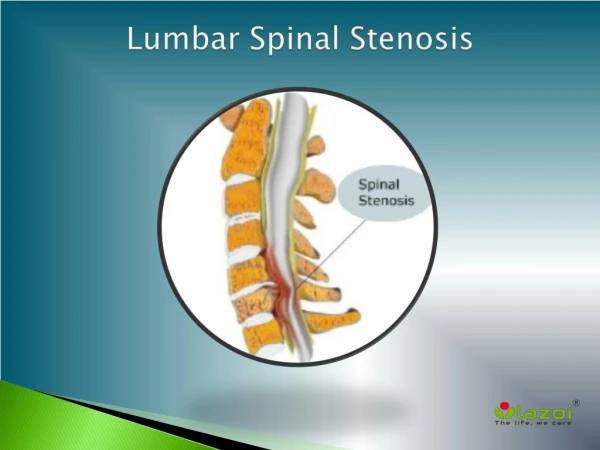
The specific parts that make up the spine 1. Vertebrae (five vertebral bodies). 2. Intervertebral Disc. 3. Facet Joint. 4. Spinal Segment. 5. Paraspinal Muscles.
Motion in the lower back Fifty percent of flexion (bending forward) occurs at the hips and fifty percent occurs at the lower spine (lower back). The motion is divided between the five motion segments in the lower back, although a disproportionate amount of the motion is at L4-L5 (lumbar segment 4 and 5) and L3-L4 (lumbar segment 3 and 4).
Spinal angles The proper assessment of the sagittal plane in normal or deformed spines remains a topic of discussion at most spine meetings today.
Normal sagittal balance Sagittal balance is the alignment of C7 to the posterior superior aspect of the sacrum on an upright radiograph. The sagittal plumb line, as drawn from center of C7, should be plus or minus 2 centimeters from the sacral promontory. The impact of pelvic obliquity and lower extremity joint angulation (hip or knee flexion) on this posture are negated.
Is sagittal balance congruent, compensated or uncompensated? • The patient's posture may or may not allow them to achieve balance in the sagittal plane. • The degree to which we assign balance to the sagittal plane is defined by our plumb line and its relationship to an axis of rotation about the hips. • This concept makes assessment of both hip positions on the standing sagittal spine film very important.
Figure (3): Method of measurement of various parameters of saggittal spinal alignment; a) Angle of thoracic kyphosis, b) angle of lumbar lordosis, c) angle of sacral inclination. (Adapted from Clinic. Rheumtol by Tuzun C 1999)
Normal sagittal balance • The central nervous system comprises a complex network of balances that maintain this posture. • Normal sagittal balance = congruent postural alignment of cervical lordosis, thoracic kyphosis and lumbar lordosis that is proportional and produces a sagittal plumb line passing from the center of C7 through the L5-S1 disc space or within 2 centimeters of the sacral promontory and through or behind the hip axis. • Overall, there is a positive correlation between thoracic kyphosis and lumbar lordosis.
Compensated (incongruent) sagittal balance • Our posture changes with age. • We tend to develop more cervical lordosis, thoracic kyphosis and less lumbar lordosis as we age. • If our spinal components are not capable of acquiring those postures, adaptive changes occur in the lower extremities.
Compensated (incongruent) sagittal balance • Compensated (incongruent) sagittal balance = disproportional change in segmental alignment, i.e. cervical, thoracic or lumbar resulting in a shift in the sagittal plumb line. • The sagittal plumb line remains within the L5-S1 disc space or within 2 centimeters of the sacral promontory by changes in knee flexion or pelvic angulation (flexion or extension) around the hips in addition to the remaining flexible spinal segments.
Uncompensated sagittal balance • Uncompensated sagittal balance = changes in segmental alignment that are not successfully accounted for by changes in flexible spinal segments, knee flexion and pelvic angulation. • This results in a shift of the sagittal plumb line either anterior or posterior to the L5-S1 disc space and greater than two centimeters from the sacral promontory. • However, the patient is able to stand up without external support.
Should routine assessment of sagittal balance include the orientation of hips and pelvis? • While the actual lumbar lordosis is important, pelvic angulation due to hip flexion or extension can significantly affect each person's spinal posture. • Jackson and Legaye have commented on the effect changes in lumbar lordosis have on the pelvis, sacrum and hips.
John and Fisher in 1994 concluded that the center of rotation was along an axis through the center of the femoral head. Hip extension, knee flexion and posterior pelvic angulation are an attempt to return the body's center of gravity to a more centered location over the hips. • Pelvic morphology can affect posture, so different measurements for pelvic morphology in the sagittal plane have been reported, including the pelvisacral angle, the pelvic incidence angle and the pelvic lordosis angle.
Lumbosacral angle: • Accounting for the wedge shape of the L5-S1 intervertebral disc • The angle between intersecting lines drawn according to the lower endplate of L5 and the superior endplate of S1. Figure (4): Methods of measuring the lumbosacral angle (2).
Pelvisacral angle: • The angle of intersection between the line from a midpoint between the center of the hip joints to the center of the superior S1 endplate and a tangent line drawn along this endplate. Figure (5):Methods of measuring sacral inclination angle (3).
Sacral Inclination: • The angle of intersection between a line drawn along the back of the S1 vertebra and the horizontal. Figure (6):Methods of measuring sacral inclination angle (1).
Radiological evaluation of lumbar intervertebral instability • Functional Radiography can demonstrate intervertebral instability or abnormal motion between two vertebrae. • Dynamic radiographs obtained in both flexion and extension prove to be a simple and reliable method to determine motion segment instability and can also indicate the lesions located in specific areas based on the "dominant lesion". Figure (7): Plain x-ray radiography for lumbar spine.
Radiological evaluation of lumbar intervertebral instability The location of the dominant lesion determines the pattern of instability: • If the dominant lesion is primary anterior restraint failure, there is posterior horizontal translation in the extension views. • If the dominant lesion is primary posterior restraint failure, there is anterior horizontal displacement in the flexion view and radiologically detectable abnormal patterns of coupling in the posterior elements.
Summary • Sagittal balance is a combination of opposing curves; cervical lordosis, thoracic kyphosis, lumbar lordosis, sacral inclination, pelvic and hip angulation (flexion or extension). • Sagittal balance has as its primary goal maintaining our center of gravity. Lumbar lordosis has the largest dampening effect on this balance.
THANK YOU