Download
1 / 16
170 likes | 449 Views
Hypothyroidism. Sarina Pasricha. Epidemiology. Hypothyroidism is five to eight times more common in women than men

E N D
Hypothyroidism SarinaPasricha
Epidemiology • Hypothyroidism is five to eight times more common in women than men • In the United States National Health and Nutrition Examination Survey (NHANES III), 13,344 people without known thyroid disease had measurements of serum TSH, T4, thyroglobulin antibodies, and thyroid peroxidase antibodies with the following results: • Hypothyroidism was found in 4.6 percent (0.3 percent overt and 4.3 percent subclinical). • Mean serum TSH concentrations were significantly lower in blacks than in whites or Mexican-Americans.
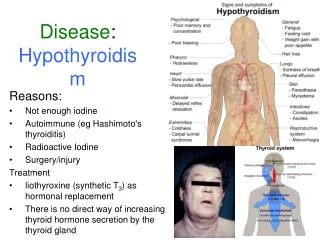
Signs and Symptoms Hoarseness Edema Coarse skin Puffy facies and loss of eyebrows Periorbital edema Enlargement of the tongue Other Decreased hearing Myalgia and paresthesia Depression Menorrhagia Arthralgia Pubertal delay Diastolic hypertension Pleural and pericardial effusions Ascites Galactorrhea Fatigue and weakness Cold intolerance Dyspnea on exertion Weight gain Cognitive dysfunction Mental retardation (infant) Constipation Growth failure Slow movement and slow speech Delayed relaxation of tendon reflexes Bradycardia Carotenemia Accumulation of matrix substances Dry skin
Clinical Scenario • 56 yo F w PMH sig for hypothyroidism presents for routine follow up to clinic. • Of note she has been feeling a little more fatigued and has gained about 2 pounds in the last month. • Current meds: Synthroid 88 mcg daily for years.
What test to order? • In a patient with no known history of hypothyroidism but clinical symptoms: • Order TSH first. If abnormal then order free T4. • Current TSH assays have detection limits of about 0.01 mU/L • Data from NHANES III has shown that normal ranges for TSH is age based • The older the pt, the higher the TSH concentration.
What test to order? • In a patient with known hypothyroidism on synthroid– order TSH to evaluate response • If serum TSH is high – increase synthroid dose • If serum TSH is low – lower synthroid dose • Exception: Pts with secondary hypothyroidism due to pituitary or hypothalamic disease who have impaired TSH production • Measure free T4 and keep it within the upper 50% of normal
Treatment of Hypothryoidism • A meta-analysis of 11 published randomized trials including 1216 patients showed that there was no benefit (fatigue, bodily pain, anxiety, depression, quality of life) of combined T4-T3 therapy • Thyroxine-triiodothyronine combination therapy versus thyroxine monotherapy for clinical hypothyroidism: meta-analysis of randomized controlled trials. • Start synthroid at a dose of 1.6 mcg/kg body weight per day • In elderly pts – start with less: 25-50 mcg daily Her TSH returned high at 4.3. Increase synthroid from 88 mcg to 100 mcg daily
Effects of Evening vs Morning Levothyroxine Intake: A Randomized Double –blind Crossover Trial • Archives of Internal Medicine; December 13/27 2010
Recommendations for our patient • Levothyroxine should be taken on an empty stomach • Do not take with coffee since coffee decreases synthroid absorbancy • Do NOT take synthroid with fiber supplements, calcium, iron, MVA, antacids or medicines that bind bile acids. • Probably recommend taking synthroid in the evening before bed
Follow-up • Symptoms should start to resolve in 2-3 weeks. • If pt still has symptoms after 2-3 weeks, then recheck TSH and Free T4 in 3 weeks. • If free T4 is still low can increase synthroid. • Re-check TSH in 6 wks after steady state is achieved. • If TSH is still high- increase synthroid by 12.5-25 mcg/day. • If you’re not changing synthroid dose, can check TSH annually.
Literature • Up to Date. 2/7/11. • Bolk et al. Effects of Evening vs Morning Levothyroxine Intake. A Randomized Double-blind Crossover Trial. Archives of Internal Medicine. 170. Dev 13/27, 2010.