Download
1 / 29
290 likes | 314 Views
A rough guide to the immune system. Dr Adrian Palfreeman Senior Clinical Scientist MRC CTU. Stem cells. Stem cells –why they matter. Neutrophil (polymorph). Multi-lobed nucleus. Commonest leucocyte (2500-7500/mm3 of blood).

E N D
A rough guide to the immune system Dr Adrian Palfreeman Senior Clinical Scientist MRC CTU
Stem cells Stem cells –why they matter
Neutrophil (polymorph) • Multi-lobed nucleus. • Commonest leucocyte (2500-7500/mm3 of blood). • A short-lived phagocytic cell whose granules contain numerous bactericidal substances. • leave the blood to go to tissues where infection or inflammation is developing
Eosinophil • A leucocyte whose large refractile granules contain a number of highly basic or ‘cationic’ proteins, • possibly important in killing larger parasites including worms. • Bind avidly to IgE-coated particles (i.e. Helminthic parasites) . • Abundant at sites of allergic reactions.
Monocyte • The largest nucleated cell of the blood (16-20μm • diameter), developing into a macrophage when it • migrates into the tissues. • Macrophage (A professional antigen presenting cell) • The principal resident phagocyte of the tissues. • Strongly phagocytic of particles and microbes. • Has receptors for Ig and complement. • CNS – “microglia” • Liver – “Kupffer cells” • Lungs – “alveolar macrophages” • Bone – “osteoclasts”
T lymphocyte (T cell) • A thymus-derived (or processed) lymphocyte. • 1500 - 4000/mm3 blood • 6-15μm diameter (red blood cell 7.2μm diam.) • 2 main subdivisions – CD8 (cytotoxic T cells) - CD4 (helper T cells)
B lymphocyte • A bone marrow- (or in birds, bursa-) derived lymphocyte, the precursor of antibody-forming cells. In foetal life, the liver may play the role of ‘bursa’. • NK (Natural Killer) cells • do not have to recognise a specific antigen before acting against it • are effective against a wide range of infectious microbes.
The 2 arms of the adaptiveimmune response 1. Humoral immunity (antibodies) 2. Cellular immunity (T-cells) • Sub-divided into T helper cells (CD4+) and • Cytotoxic T cells (CD8+)
CD4 Lymphocytes (T helper cells) • coordinate much of the immune response to micro-organisms • help B-cells respond to foreign proteins • secrete substances that enable CD8 T-cells to proliferate • activate macrophages so that they can kill certain organisms, including some organisms associated HIV infection.
CD8 Lymphocytes (Cytotoxic T cells) • kill cells in the body identified as abnormal or foreign • tumour cells • cells that have been infected by viruses.
How does HIV reduce CD4 Cells? • Increased turnover of cells in response to infection • Trapping of HIV in lymph nodes • Shortened survival of CD4 cells • Reduced production of new cells • Reduction of T cell progenitor production from bone marrow
Sites of theprincipallymphoid tissueswithin the humanbody.Primary lymphoidorgansSecondary lymphoidorgans
Human lymphoid organsPrimary lymphoidorgansSecondary lymphoidorgans
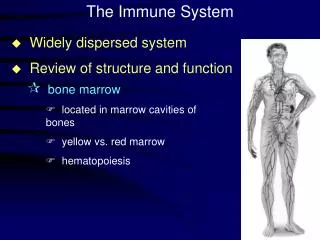
Lymphoid tissues • Immune system compartmentalised into organs/tissues. • Funtionally unified via blood and lymph systems. • Lymphocytes recirculate. • In total, equivalent in weight to brain or liver. • Primary lymphoid organs • Bone marrow where T and B lymphocytes are made. • Thymus where T lymphocytes mature/are selected. • Secondary lymphoid organs • e.g. spleen, lymph nodes and Peyer’s patches. • Contain T cells, B cells, antigen presenting cells (APCs)
T cell precursors(thymocytes) migratefrom the bone marrowto the thymus to mature. Mature T cells leave the thymus and migrate to secondary lymphoid tissues where they may encounter foreign antigen.
Thymus Lobules show - a lymphocyte-dense outer cortex - an inner lighter-staining medulla. Stromal framework with specialised epithelial cells, DCs and macrophages (APCs). T cell precursors arrive from the bone marrow. Cortex and medulla ‘educate’ thymocytes into mature, competent T cells (1 to 3% of T cells survive education). Mature T cells are released into the peripheral circulation.
THYMUSDevelopingthymocytesoccupy theinterstices ofan extensivenetwork ofepithelial cells
Clusters of Differentiation (CD) • CD3 T cells • CD4 Helper T cells • CD8 Cytotoxic T cells • CD16 Macrophages • CD19 B cells
Circulatinglymphocytesmeetlymph-bornepathogensin draininglymph nodes.
Cytokines • Il2 stimulates division of B and T cells and killing of HIV infected cells by NK cells • IL2 levels reduced in HIV infection
IL2 • Does administration of IL2 help? • Raises CD4 numbers • Significant side effects • Injectable • Short term benefit in clinical trials • Does it reduce mortality and morbidity in the long term?
Summary • B cells recognise antigens (antigenic epitopes) via their monomeric IgM receptor • T cells recognise antigens (small peptides)via the T cell receptor (TCR) which is always associated at the cell surface with CD3 11 • The monomeric B cell receptor (and, in fact, all antibodies) recognise antigens in solution – in their native (folded) state • The TCR does not recognise soluble antigens but only small antigenic peptides associated with the Major Histocompatibility (MHC) molecules I & II • For a T cell or B cell to be activated 2 appropriate signals are always required • T cells need binding of the TCR to peptide/MHC plus specific cytokines from the APC (notably IL- 1 and IL-2) and interaction between B7 and CD28 • B cells need binding of mIgM surface receptor plus signals from TH cells (notably IL-4 and IL- 10) and interaction of CD40/CD40L. • This process has evolved to prevent unwanted activation of immune cells which can lead to harmful responses such as allergies and autoimmunity