Download
1 / 15
150 likes | 342 Views
Detection of Pneumocystis carinii in rat colonies by PCR and Serology. Vandana S. Dole, Michelle L. Wunderlich, Barry A. Bronson, Robert L. Brouillette, Rajeev K. Dhawan, William R. Shek, Kenneth S. Henderson *. Background.

E N D
Detection of Pneumocystis carinii in rat colonies by PCR and Serology • Vandana S. Dole, Michelle L. Wunderlich, Barry A. Bronson, Robert L. Brouillette, Rajeev K. Dhawan, William R. Shek, Kenneth S. Henderson*
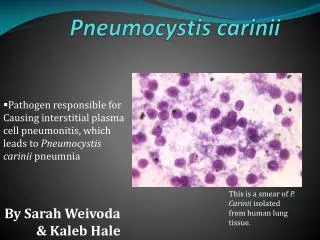
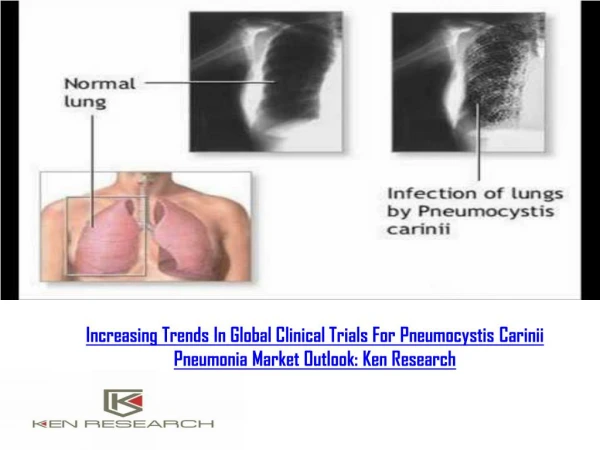
Background • Elwell, et. al. 1997 described distinct lung lesions characterized by lymphohistiocytic interstitial pneumonia and perivascular lymphocytic cuffing in laboratory rats • Albers et. al. (Vet. Path, 2009), published evidence supporting it was caused by a transmittable agent and suggested diagnostic histological criteria for infectious interstitial pneumonia • Pneumocystis carinii identified as the etiologic agent for the lesions (Livingston et. al., Comp. Med. 2011) and that it was not a virus as was previously reported • Our laboratory corroborated the identity of the etiology with the intent to improve methods for screening through a series of investigations (NAALAS, 2010).
Identification of the etiology was required so that more efficient, sensitive, and specific methods of screening could be developed • For more than a decade, only histopathology was available for screening • Labor intensive • Small window of opportunity for detection of lesions, which begin to resolve 5-6 weeks after the initial peak • Albers et. al. study • Naïve rats introduced into infected breeding colony • Exposed to 50% soiled bedding from rats 8 weeks of age
Overlay of histology scores with quantitative PCR, and IFA serum titration data obtained for archived samples • Genome copy numbers (PCR) increases slowly and the peak coincides with lung lesions • Henderson, et. al., 2010, NAALAS Seroconversion occurs when PCR and lesion peak Copy numbers decrease and lesions begin to resolve shortly after seroconversion
Detection challenges for P. carinii • Pneumocystis transmission is not efficient • Pneumocystis researchers commonly rely on intra-tracheal inoculation for consistent infection even for immunodeficient or immunosuppressed models • Rate of infection is related to dose • Seroconversion by exposure to bedding or open top cage environments is delayed compared to contact exposure (Henderson, et. al., submitted for publication) • 4.5 day doubling time (Aliouate, et. al., 1999) • Seroconversion occurs ~ 7 weeks after rats received 50% dirty bedding in an open-top cage barrier room (Henderson, et. al., NAALAS, 2010)
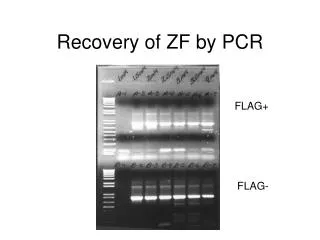
Challenge for PCR Henderson, et. al., submitted for publication • CD rats exposed by contact to 2- week pre-exposed RNU rats • Different sample types evaluated by PCR • Lung is the best PCR sample • Provides the earliest and largest window of detection • Oral swabs (ante-mortem) are not suitable • Same for nasal swabs and fecal pellets (data not shown)
Challenges for Serology Seropositive Seronegative • Indirect immunofluorescence assay (IFA) • Requires propagation of the organism • Can not be continuously passaged in culture • Requires propagation in rats for antigen • Too labor intensive for primary screen • P. carinii MFIA development • Recombinant antigen (Dhawan, et. al., NAALAS, 2011) • Provides a high-throughput multiplexed screening of samples
Endemically infected barrier rooms Pathology/MFIA Scores • Henderson, et. al., 2010, NAALAS • Sprague Dawley Rats (N=6/age group) • MFIA detects low maternal antibodies in 3 wk rats • Antibodies mostly absent in 7-8 wk rats, but 80% are PCR + • All 10-12 wk rats were PCR positive and seroconversion is detected in 50% of rats • At 29-30 weeks all rats are MFIA positive.
10 week time course study: CD rats exposed by contact Pathology/MFIA Scores • Henderson, et. al., 2010, NAALAS Similar pattern as observed for Albers et. al. study Time line was ~2-week earlier
Summary of test results for rats from endemically infected barrier room and the contact time-course study • Suggests that serology or PCR alone may not provide comprehensive detection a -Data are from tests of 132 contact-exposed CD rats in transmission experiments II and IV and of 36 SD rats in the enzootically infected barrier-room breeding colony (Fig. 9). b -Positive cutoffs: ≥ 5 Pneumocystis DNA copies/mg lung by qPCR and antibody titer ≥ 0.5 Log10 by P. carinii IFA. c - Different Greek letter superscripts denote significant differences (P <0.01, Cochran test with pair-wise comparisons and the McNemar’s test)
Question: Could bedding sentinel infection be delayed and seroconversion not detected by serology if the infectious dose is too low? • Based on our concerns, rats submitted to Research Animal Diagnostic Services (RADS) for routine health monitoring since January 2011 were monitored by both MFIA and PCR for P. carinii • Data from the RADS Internet Laboratory Information Management System (ILIMS) was extracted to determine prevalence and to compare PCR and MFIA screening methods
Independent assay screening: Samples submitted for PCR or MFIA External samples received by RADS 1/2011 – 5/2011
Parallel screening of rats by PCR and MFIA n=599, distribution of 131 positives Pneumocystis PCR and P. carinii MFIA results were compared for rats submitted to RADS for routine health monitoring Combined Prevalence = 20%: Compare to 6% reported based on lung screening by histology (Pritchett-Corning, et. al., 2009)
Examples of rat submissions • Detection by one method or the other is not uncommon within sponsor submissions • Other variables that may contribute to delayed seroconversion in bedding sentinels • Prevalence on the rack • Stage of infection in study rats • Amount of bedding that is transferred
Summary P. carinii is a highly prevalent infectious agent in laboratory rats P. carinii replicates slowly and is best spread by direct contact Our previous studies suggest that that the timeline for sero-conversion is dose dependent Serology and PCR together are important for detection of P. carinii