Download
1 / 29
410 likes | 1.14k Views
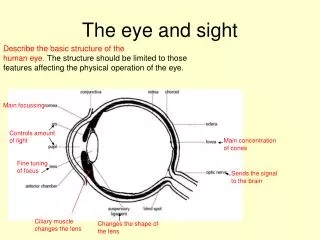
Hypertension and the Eye. John B. Crane, O.D. Clinical Assistant Professor College of Optometry University of Missouri- St. Louis Member, Missouri Diabetes Advisory Board. The Basics. Most people with hypertension never develop vision problems due to their disease

E N D
Hypertension and the Eye John B. Crane, O.D. Clinical Assistant Professor College of Optometry University of Missouri- St. Louis Member, Missouri Diabetes Advisory Board
The Basics • Most people with hypertension never develop vision problems due to their disease • If vision is directly affected by hypertension, usually the patient’s life is at risk (malignant hypertension) • Long term reduced vision due to direct and indirect effects of hypertension is fairly rare • “Hypertensive Retinopathy” refers to the chronic and acute retinal signs that occur in the retina due to hypertension
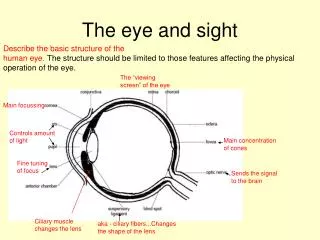
Hypertensive Retinopathy-What is it? • Findings all stem from changes induced in the retinal microvasculature by hypertension. Similar changes occur elsewhere in the body. • Arteriosclerosis • Chronic abnormal thickening and hardening of medium and large arterial walls resulting in artery straightening & loss of artery elasticity • Arteriolosclerosis • Thickening of the inner wall of small arteries (arterioles) by fatty deposits resulting in obstructed blood flow
Hypertensive Retinopathy-Clinical Findings • Chronic signs: Arterial narrowing (“attenuation”), artery-vein crossing changes with venous constriction and banking, artery “straightening”, arteriolar color changes • Acute signs: • Cotton-wool spots (diastolic usually >110) • Flame hemorrhages • Optic disc edema (BP usually >250/150) • The garden hose analogy
Indirect Ocular Associations with Hypertension • Hypertensive patients have a higher risk of: • Branch retinal vein occlusion • Ischemic optic neuropathy • Retinal macroaneurysm • Severe diabetic eye complications
Clinical Studies • Those with relatively narrowed arterioles are twice as likely to develop severe hypertension in 5 years as people with relatively wider arterioles (Hypertension: Journal of the American Heart Association) • Suggests that structural microvascular changes, visible in the eye, may precede development of severe hypertension • Therefore, effective treatment for early hypertension may need to specifically target the microcirculation • Also suggests that visible structural changes in the retinal arterioles could be a better measure of long term risk than blood pressure measurements (which can vary significantly)
Clinical Studies • Those who are regular users of aspirin (daily to weekly use) have wider retinal arteriole diameters than nonusers, suggesting that aspirin affects small retinal vessels in a measurable way (ARVO, May 2005) • Narrow vessels are associated with stroke, heart attack, heart failure, and peripheral vascular disease • Unknown whether the changes seen in the eye are also seen in the brain, heart, and other organs • Ongoing research will try to determine how this new knowledge can be applied to help reduce the risk of organ damage related to hypertension
36 yo AAF cc: “blur at all distances” OD>OS HPI: location: OD floater? “blurry spot that moves” OS “one side blurry” duration: x 1 wk timing: “all of the time” severity: severe assoc s/s: +photophobia x 1wk., itch, burn, eyestrain while reading x 1 wk HA: 2 per month x 3 months timing varies, sharp generalized pain at temples, pain rating 8, Excedrin helps
POHx: unremarkable FOHx: unremarkable ROS: +HTN- had baby 3 months previously, hospitalized for 70 days prior to delivery due to BP spikes and BS fluctuations +IDDM x 11 yrs., pt. reports blood sugar kept at 120 mg/dL or lower; ?A1C Meds: Insulin Lisinopril 20mg qd
36 y.o. AAM • cc: “Blurry vision in left eye” • Entering VA c Rx: OD 20/20-3 OS 20/400
2 weeks later: • Had CT to r/o CVA, secondary to right-sided weakness, visual disturbance, and incontinence • Found: • “Intraventricular hemorrhage and intraparenchymal hemorrhage including the left basal ganglion and left periventricular white matter areas” • “Left to right shift” • “Edema of the left hemisphere • In other words: The patient stroked out…
10 days later: • Admitted to neuro-intensive care • Patient found to have “no purposeful movements” upon arrival • Lab history includes toxicity screen positive for cocaine • BP: 198/109 • Assessment: • “Bleed site is likely the left thalamus” • Plan: • “Patient has extremely poor prognosis”
“Pt. nonresponsive to verbal or painful stimuli. No spontaneous heart tones or respirations. Pupils fixed and dilated.” • “Death pronounced at 13:28, family at bedside, chaplain present.”