Download
1 / 40
410 likes | 477 Views
Kidneys and Hypertension. Kerala Institute of Medical Sciences. Epidemiology. Single most preventable cause of premature death in developed countries. ½ of those with hypertension have not been diagnosed. ½ of those with diagnosis are not on treatment.

E N D
Kidneys and Hypertension Kerala Institute of Medical Sciences
Epidemiology • Single most preventable cause of premature death in developed countries. • ½ of those with hypertension have not been diagnosed. • ½ of those with diagnosis are not on treatment. • ½ of those on treatment do not have adequate control.
Target organ damage • Heart- LVH, IHD, LVD,CCF. • Brain- Stroke, TIA,Vasular dementia. • Chronic Kidney Disease. • Peripheral arterial disease. • Retinopathy.
Pathogenesis. • No one gene is not responsible. • Studies shows that several difft genes may have an effect on BP. • RARE SINGLE GENE CAUSES OF HTN HAVE BEEN IDENTIFIED.
Liddle’s Syndrome. • Autosomal dominant inheritance. • Increased sodium retention. • Hypokalemia. • Metabolic alkalosis. • Suppressed aldosterone level.
Liddle’s • Diagnosis- young hypertensive, with positive family history, mild hypokalemia, mild metabolic alkalosis,decreased renin, decreased aldosteron level.
Liddle’s – Treatment. • Low salt diet. • Amiloride or triamterene.
Other single gene causes of Hypertension. • Glucocorticoid remediable aldosteronism. • Syndrome of minerelocorticoid excess. • Pheochromocytoma - may occur with MEN type 2, Von Hippel Lindau disease, Neurofibromatosis type 1.
MEN 2 –pheochromocytoma, medullary carcinoma of thyroid, hyperparathyroidism. • Von Hippel Lindau- Pheochromocytoma,renal cell carcinoma, cerebellar and retinal hemangioblastoma.
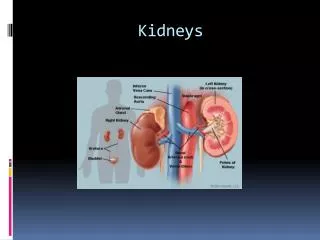
Renin angiotensin system • Renin –secreted by the juxtaglomerular apparatus. • It converts angiotensinogen (inactive) to angiotensin 1 .It then converts to angiotensin 2 by ACE. • Increased renin – RAS, Renal cell carcinoma.and rarely some renin secreting tumours.
Actions of angiotensin ii • Arteriolar vasoconstriction. • Efferent arteriolar vasocnstriction. • Aldosterone secretion. • Epinephrine release (adrenaline). • Smoothmuscle hypertrophy. • Inhibit renin release (negative feed back). • Myocardial growth.
Aldosterone. • Synthesis mainly in the zona glomerulosa of the adrenal cortex. • Regulated by the RAS. Or by the electrolyte imbalance. • Hyperkalemia and low salt intake promote aldosterone synthesis.
Other pathogenesis • Arterial stiffness – Aging , DM, Kidney disease. • Sympathetic nervous system- Activation associated with sudden rise in BP.- By increasing stroke volume, HR , systemic vascular resistance and activation of RAS.
White coat hypertension. • Clinic BP high but Ambulatory BP normal. • Consider when BP appears elevated but no target organ damage. • May be a precursor of sustained HTN.
Initial assessment • Duration of HTN • Othere CVD risk factors. • Anything to suggest secondary HTN. (Age <30, sudden onset, presents as malignant HTN, sudden deterioration in BP control, resistant HTN (>3drugs)
Initial evaluation • Other contributory factors like –drugs, overweight, Excess ETOH, excess salt intake, Lack of exercise, Environmental stress, smoking. • Evidence of Complications- stroke, TIA, Carotid bruit, IHD, CCF, Cardiomegaly,PVD, Hypertensive retinopathy, Renal impairment, proteinuria, Sexual dysfunction,
Initial Evaluation. • Previous drug treatment and side effects. • Contraindication to specific drugs. • Family history
Initial basic investigations. • Urine R/E • Fasting lipids and sugar. • ECG for LVH. • Urea/ Cr ,H/H , Microalbuminuria, ECHO, CRP , Urea, Creatinine – these are all desirable tests.
Secondary Hypertension • Primary renal disease- increased creatinine, proteinuria, hematuria. • A/C or c/c glomerulonephritis.,ADPCKD,Obstructive uropathy • HTN may be a cause or effect in CKD.But treat aggressively. Target BP 120/70- 130/80.
What Drug in CKD • In all proteinuric renal disease ACEI and ARB has a beneficial role. • Dcreases intraglomerular pressure and thus reduce proteinuria. • Dual blockade with ACEI and ARB is a useful combination.
In CKD • Expect the need of 3 meds. • First life style modification. • If proteinuria ACEI. • If fluid overload diuretics. • If persistant proteinuria add ARB. • If BP still high dihydropyridines- Nifedipine, Amlodipine.
Next step usually B blockers. • Still not controlled centrally acting agents – catapress (clonidine) • Next preferable agent- Alpha blocker. • Last vascular smooth muscle relaxent- Minixidil.
Remember side effects. • Hyperkalemia (ACE, ARB) • Fluid retension (Amlodipine) • Bradycardias (B blocker, Clonidine) • Massive fluid overload and Tachycardia (minixidil)
Renal artery stenosis. • Atherosclerotic or fibromuscular dysplasia as aetiology. • Clinically difficult to control HTN, • Renal dysfuntion • Resistant fluid retention. • Worsening Cr with ACEI or ARB.
Investigations • US Kidneys- assymmetry. • Doppler of renal arteries. • Captopril renogram – affected kidney may show a 30% decline in function. • MRA. • Angiogram .secure diagnosis and allow intervention.
Treatment - in Atheroslerotic RAS • Modify risk factors. • Control BP with loop diretics, calcium channel blockers, centrally acting agents, B blockers, • Tratement by angioplasty and stenting OR surgery.
Indications for surgery • Single kidney with stenosis. • Bilatteral RAS. • Uncontrolled BP/ flash pulm oedema. • Rapidly deteriorating kidney function. • Meanigfull nephron mass in the kidneys.
Fibromuscular dysplasia. • Otherwise healthy young women aged 15-50 yrs. • Angiography with “string of beads” pattern • Angioplasy is the treatment.
Primary hyperaldosteronism • Aldosterone act on the distal tubule and cause increased Na retention and increased urinary K and H wastage. • Causes- Conns syndrome ( aldosterone producing adrenal adenoma), bilatteral adrenal hyperplasia.,adrenal carcinoma.
Diagnosis • Low serum K. • Renal K wasting. • Increased aldosterone and low renin level. • Adrenal CT or MRI to locate tumour. • Treatment Spironolactone/+amiloride.
Secondary hyper aldosteronism • Secondary to increased renin.- in RAS, Renal infarct, CCF, renal trauma, renin secreting tumours.
Pheochromocytoma • Very rare. • Paroxysmal symptoms.(Head ache, palpitation, sweating). • Usual screening tests – 24 hr urine for VMA and catecholamines. • Adenoma or carcinoma (rarely) can be located by MIBG scanning.
Miscellaneous causes. • Obstructive sleep apnoea. • Thyrotoxicosis. • Acute intermittent porphyria. • Alcohol withdrawal.
HTN in pregnancy • Pregnancy induced HTN –HTN after 20 wks of gestation. • HTN complicating pregnancy – HTN before 20 weeks of gestation. • Transient HTN – not seen in repeated measurements.
Treatment • Reduction in Maternal BP can reduce the fetal blood flow, so can aggrevate the IUGR. • If treatment needed consider Methyldopa 250 mg bd up to 750 mg tid. Or Labetolol 50 titrate up to 100 mg bd. Atenolol may be given but be aware of neonatal brady cardia.
Nifedipine can be used , but no sufficient data to use amlodipine routinely. • Another alternative is oral Hydralazine 50 mg BD and may increase upto 100 mg tds.
avoid diuretics. • ACEI, ARB, CLONIDINE, MINOXIDIL, NEWER alpha and B blockers are contraindicated in preganacy or too little experience with these medications.
Avoid reducing BP suddenly. • If IV antihypertensives needed labetolol,and hydralazine are the choices. • Labetolol 20 mg slow IV bolus and upto a cumulative dose od 300 mg( may rpt doses every 10 minutes) .
Labetolol infusion upto a maximum of 160 mg/hr. • Monitor fetal HR. • Hydralazine 5 mg bolus over 5 minutes and repeat every 20 minutes upto 20 mg. • Hydralazine infusion start with 2mg/hr maximum 20 mg/hr.