Download
1 / 17
170 likes | 1.21k Views
Right ventricle infarction. Dr. P Kruger 2004. General Pathophysiology RCA supply and occlusion Clinical Special examinations Treatment Conclusions Examples. General. RVI mostly associated with inferior MI, seldom isolated RVI 30-50% of Inferior MI 10-15% haemodynamic unstable

E N D
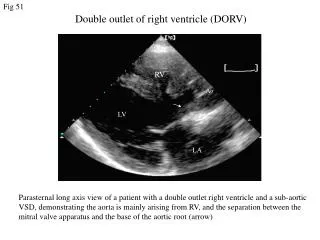
Right ventricle infarction Dr. P Kruger 2004
General • Pathophysiology • RCA supply and occlusion • Clinical • Special examinations • Treatment • Conclusions • Examples
General • RVI mostly associated with inferior MI, seldom isolated RVI • 30-50% of Inferior MI • 10-15% haemodynamic unstable • Higher morbidity and mortality than inferior MI • Mortality 25-30% - Inferior mi + RVI = 31% - Inferior mi – RVI = 6% • Spectrum of disease: Asymptomatic mild RV dysfunction to cardiogenic shock
Pathophysiology • RV is a thin walled chamber that function at low O2 demands. • RV is a low-volume pressure pump, its contractility is highly dependent on diastolic pressure. • It’s perfused throughout the cardiac cycle in both systole and diastole • Its ability to extract O2 is increased during haemodynamic stress • Collateral blood supply ( esp. anterior wall of RV) • All of these factors make the RV less susceptible to infarction than the LV
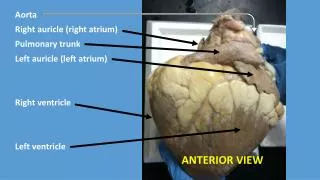
Right coronary artery • Posterior descending branch - Inferior and posterior wall of RV • Marginal branches - Lateral wall of RV • Conus branch - Anterior wall ( also supplied by L descending artery , moderator branch)
Right coronary artery occlusion • Mostly ateriosclerotic occlusion of proximal RCA • Direct correlation between anatomic site of RCA occlusion and extent of RVI. • More proximal occlusion causes a larger RVI • Proximal to RV occlusion of RCA causes: RV free wall injury compromises blood supply to SA node, atrium and AV node sinus brady, atrial infarction, AF, AV block.
Clinical • Classic triad of : 1. Raised JVP 2. Clear lung fields 3. Hypotension
Special investigations CXR BLOODS ECG Inferior MI - ST elevation in II, III, aVF - With/without abnormal Q waves Right-sided ECG - ST elevation in lead VR - ST disappear after 10 hours of onset of pain - ST more than 1mm/ 0,1mV
Treatment • General measurements • Recognition • Reperfusion • Volume loading • Inotropic support • Rate and rhythm control • Complications
RVI should be considered in patients with sensitivity to preload-reducing agents such as diuretics, nitrates, morphine • All patients with Inferior MI considered as RVI until proven otherwise