Download
1 / 38
420 likes | 580 Views
Gain insight into hemostasis mechanisms and coagulation cascade in newborns. Explore anticoagulants, HIT, DIC, and hemostatic agents. Learn about differences between neonatal and adult coagulation.

E N D
Coagulation Cascade of the Newborn Sylvia del Castillo, MD Clinical Associate Professor of Pediatrics USC Keck School of Medicine Medical Director, Cardiothoracic Intensive Care Unit Children’s Hospital Los Angeles
Objectives • Understand balance between hemostasis and bleeding • Familiarize ourselves with various Anticoagulants and their laboratory studies • Heparin • Understand the concept of HIT • Warfarin • Aspirin • Understand the mechanism of DIC • Understand the use of hemostatic agents
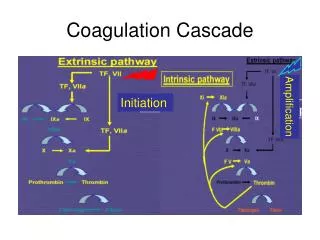
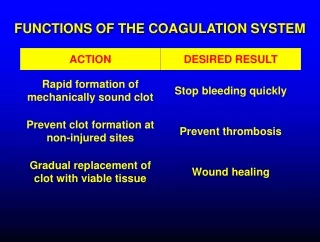
What is Hemostasis? • A balance of pro and anti-coagulation to protect us from uncontrolled bleeding secondary to vessel injury while at the same time preventing excessive clotting….. • Primary: at site of injury, adhesion, activation and aggregation of platelets results in formation of platelet plug • Secondary: Activation of the coagulation cascade results in formation of fibrin that stabilizes the platelet plug
Hemostasis Exogenous Agent Endogenous Agent VASCULAR INJURY Exposed subendothelium von Willebrand factor Tissue factor Thrombin TXA2 Vasoconstriction Platelet Adhesion & Aggregation Coagulation PL, PF TXA2 Serotonin HEMOSTASIS
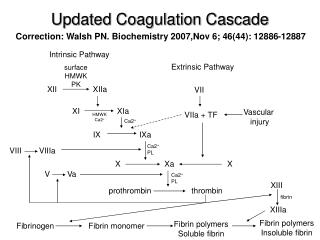
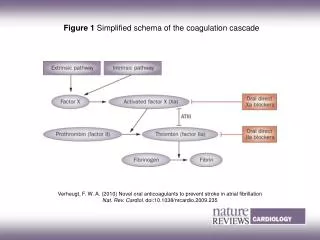
PTT = intrinsic pathway (PiTT) PT = extrinsic pathway (PeT)
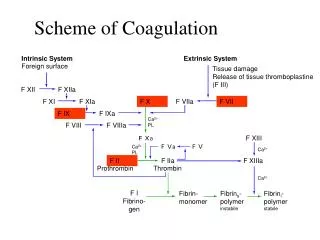
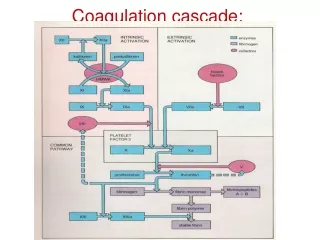
Coagulation Pathways EXTRINSIC PATHWAY INTRINSIC PATHWAY Injury 12 12a 11 11a 7 + Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
Neonates vs. Adults • Platelet number and volume similar • Factor V lower in pre-term neonates • Factor VIII higher in pre-term neonates • Pre-term and term neonates born with less amount of all procoagulant factors and vitamin K dependent factors • AT-III levels in the 1st 3 months of life lower than in adults
Revel-Vilk. The conundrum of neonatal coagulopathy. Hematology 2012
https://www.google.com/search?safe=off&biw=1536&bih=775&tbm=isch&sa=1&ei=iymCWsSZL9fIjwPSgbyADA&q=coagulation+cascade+cartoons&oq=coagulation+cascade+cartoons&gs_l=psy-ab.3...2966.9225.0.9633.30.15.1.12.12.0.151.1523.7j7.14.0....0...1c.1.64.psy-ab..3.26.1722...0j0i67k1j0i24k1.0.1VO-LU5fuL8#imgdii=V2BwoqkyLvGhAM:&imgrc=cpGxvavfr8fGNM:https://www.google.com/search?safe=off&biw=1536&bih=775&tbm=isch&sa=1&ei=iymCWsSZL9fIjwPSgbyADA&q=coagulation+cascade+cartoons&oq=coagulation+cascade+cartoons&gs_l=psy-ab.3...2966.9225.0.9633.30.15.1.12.12.0.151.1523.7j7.14.0....0...1c.1.64.psy-ab..3.26.1722...0j0i67k1j0i24k1.0.1VO-LU5fuL8#imgdii=V2BwoqkyLvGhAM:&imgrc=cpGxvavfr8fGNM:
Anticoagulants • Heparin • IV or subcutaneous (SQ) • Onset of action • IV – immediate • SQ– 20-30 minutes • Half-life • 30-60 minutes • Usual dose • Bolus – 50-100 units/kg • Drip – 15-45 units/kg/hr • AntiThrombin III (AT-III) • Neutralizes enzymatic activity of Thrombin • Affects Factors IIa, IXa, Xa
Where to measure the effect? EXTRINSIC PATHWAY INTRINSIC PATHWAY Injury 12 12a 11 11a 7 + Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
Anticoagulation Studies • Activated Clotting Time: ACT • Number of seconds it takes for a blood clot to form • Tests the intrinsic and common pathways • 70 – 120 seconds without heparin • 180 – 240 seconds with heparin • Less sensitive than PTT • Results can be affected by thrombocytopenia and hemodilution • Only run on fresh whole blood and only a side test
Anticoagulation Studies • Partial Thromboplastin Time : PTT • Tests intrinsic and common pathways • Not affected by platelet count • Can be run on fresh or citrated blood samples (ie can be run within 2 hours of collection) • PTT 25 – 40 seconds • “a”PTT: an activator is added to the blood sample that speeds up clotting time • Heparinized PTT = 1.5 – 2.5 x normal PTT
Anti-Coagulation with Heparin EXTRINSIC PATHWAY INTRINSIC PATHWAY Injury 12 12a 11 11a 7 + Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a PTT 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
Anti-Xa EXTRINSIC PATHWAY INTRINSIC PATHWAY Injury 12 12a 11 11a 7 +Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
Heparin-Induced Thrombocytopenia (HIT) Courtesy of Dr. John Kelton
HIT Diagnostic Criteria • Decreased platelet count during heparin therapy • Absence of other causes • Increasing heparin resistance • Platelet count rebound after heparin is stopped • Confirm heparin-platelet antibody by in vitro testing • Antibody assay (ELISA) • Serotonin release assay
Warfarin • Oral • Onset of action • First effect - 1 day • Peak effect - 2-5 days • Half-life • 20-60 hours • Usual dose • 0.1-0.2 mg/kg
Anti-Coagulation with Warfarin EXTRINSIC PATHWAY INTRINSIC PATHWAY Injury 12 12a 11 11a 7 + Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a INR/PT COMMON PATHWAY 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
What is PT/INR? • Prothrombin Time: PT • Normal 9 – 15 seconds • International Normalized Ratio: INR • Ratio of the patient’s PT / normal PT indexed to a standardized sensitivity index • Normal ratio < 1.5 (0.8 – 1.2) • Both evaluate the extrinsic pathway of coagulation
ASPIRIN • Oral • Onset of action • 1-7 minutes • Anti-platelet effect • About 4 days • Usual dose • 5 mg/kg
Thromboelastography (TEG) R = reaction time; K = the speed of clot formation; MA = clot strength and 80% of MA is derived from platelet function
PFA-100 TEG
The previous agents KEEP you from clotting, but what if you’ve already formed a clot? TPA= tissue plasminogen activator
Disseminated Intravascular Coagulation
What is D-Dimer? A small protein fragment that results after a clot is degraded by fibrinolysis. Two “D” fragments of the fibrin joined by a cross link. https://en.wikipedia.org/wiki/D-dimer
Liver failure or DIC? • Vitamin K dependent clotting factors • II • VII • IX • X • Protein C • Protein S • How do you tell the difference between liver failure and DIC? • Check non liver dependent coagulation factors • VIII and V
FFP vs Cryoprecipitate • FFP • All coagulation factors • Relatively large volume (10ml/kg) • Cryoprecipitate • Firbrinogen • Smaller volume • Factor VIII • Large VWF • Factor XIII
Aminocaproic Acid • Antifibrinolytic agent • Useful in mucus membrane bleeding and post-surgical bleeding • IV and topical • Onset of action • 1 – 72 hours • Half life • 1 – 5 hours • Usual dose • 33.3mg/kg/hr
Other Agents INTRINSIC PATHWAY EXTRINSIC PATHWAY Injury 12 12a 11 11a 7 + Thromboplastin 9a 9 8 Lipid, Ca Ca 10 10 10a COMMON PATHWAY 13 5 Lipid, Ca Prothrombin (2) Thrombin (2a) Fibrinogen Fibrin Fibrin polymer 13a Clot
SUMMARY • Intrinsic Pathway longer (PiTT) • Extrinsic Pathway Shorter (PeT) • Common Pathway has Factor X as the center • In DIC, ALL factors and platelets are consumed
Thank you https://www.youtube.com/watch?v=SGzp9wqeu84