Download
1 / 24
300 likes | 859 Views
LASSA FEVER ( an epidemic prone haemorrhagic fever ). BY DR. JAMES O. BAMIDELE, MD; FMCPH Associate Professor of Public Health. What is Lassa Fever?. An acute viral illness that was discovered in 1969 when two missionary nurses died in Nigeria;

E N D
LASSA FEVER(an epidemic prone haemorrhagic fever) BY DR. JAMES O. BAMIDELE, MD; FMCPH Associate Professor of Public Health
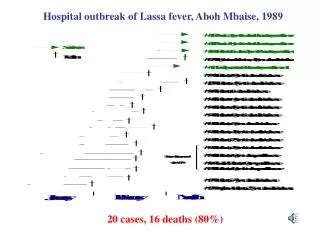
What is Lassa Fever? • An acute viral illness that was discovered in 1969 when two missionary nurses died in Nigeria; • The virus was named LASSA after the town in Nigeria where the first case originated; • The virus is of the family Arenaviridae – a single-stranded RNA virus and is ZOONOTIC or animal-borne.
Where is Lassa fever found? • Mainly in West African countries of: Guinea, Liberia, sierra Leone and Nigeria; • In these areas where the disease is endemic (i.e. constantly present), LF is a significant cause of morbidity and mortality; • It is mild in about 80% of people infected with the virus, while the remaining 20% have a severe multisystem disease
Epidemic prone LF disease!!! • LF is associated with occasional epidemics, during which the case-fatality rate can reach 50%; • Lassa virus infections per year in West Africa is estimated at 100,000 – 300,000, with approximately 5,000 deaths; • This estimate is crude since surveillance for cases is not uniformly performed.
In what animal host is Lassa virus maintained? • The reservoir, or host, of Lassa virus is a rodent known as “multimammate rat” of the genus Mastomys; there are many species! • Mastomys rodents breed very frequently, produce large numbers of offspring, and are numerous in the savannahs and forests of West, Central and East Africa; • Mastomys generally readily colonize human homes!!!!!
How do humans get Lassa fever? • The Mastomys rodents shed the virus in urine and droppings; • Therefore, the virus can be transmitted through direct contact with these materials, through touching objects or eating food contaminated with these materials, or through cuts or sores; • Mastomysrodents often live in and around homes and scavenge on human food remains or poorly stored food, transmission of this sort is common;
How do humans get LF conts: • A person may inhales tiny particles in the air contaminated with rodent excretions – aerosol or airborne transmission; • Mastomys rodents are sometimes consumed as a food source, therefore infection may occur via direct contact when they are caught and prepared for food; • LF may occur when a person comes into contact with virus in the blood, tissue, secretions of an individual infected with the Lassa virus e.g. In village and health care settings. • Through contaminated medical equipment, such as re-used needles (this is called nosocomial transmission).
What are the symptoms of LF? • Signs and symptoms of LF typically occur 1-3 weeks (IP ranges from 6-21 days) after the patient comes into contact with the virus; • Fever, retrosternal pain (pain behind the chest wall), sore throat, back pain, cough, abdominal pain, vomiting, diarrhoea, conjuctivitis, facial swelling, proteinuria (protein in urine), and mucosal bleeding. • Neurological problems include: hearing loss, tremors, and encephalitis
Laboratory diagnosis • Most often diagnosed by using enzyme-linked immunosorbent serologic assays (ELISA); • It detect IgM and IgG antibodies as well as Lassa antigen; • The virus itself may be cultured in 7 to 10 days;
Complications after recovery? • The most common complication of LF is deafness - in about one-third of cases; and severity of the disease does not affect this complication as deafness may develop in mild as well as in severe cases; • Spontaneous abortion is another serious complication;
Management of Lassa Fever • RIBAVIRIN, an antiviral drug, has been used with success in LF patients; • It has been shown to be most effective when given early in the course of the illness; • Also supportive care consisting of maintenance of appropriate fluid and electrolyte balance, oxygenation and blood pressure monitoring, as well as treatment of any other complication!
Groups are at risk for getting LF? • Lassa fever occurs in all age groups and in both men and women!!! However, risk is greater among: - Those who live or visit areas with a high population of Mastomys rodents infected with Lassa virus; - Those exposed to infected humans – hospital staff especially those attending directly to the LF patient and his blood, urine samples, etc; (However, hospital staff are not at great risk for infection as long as protective measures [universal precautions] are taken)
Prevention of Lassa Fever • Humans can be prevented by avoiding contact with Mastomys rodents; • Putting food away in rodent-proof containers; • Keeping the home clean help to discourage rodents from entering homes; • Trapping in and around home can help reduce rodent populations;
Prevention of Lassa Fever (contd) • When caring for patients with LF, taking preventive precautions against contact with patient secretions; • Use of barrier nursing methods: wearing protective clothing, such as masks, gloves, gowns, and goggles; • Using infection control measures: e.g. complete equipment sterilization; • Isolation of infected patients from contact with unprotected persons until the disease has run its course.
Challenges in the diagnosis and treatment of LF • Symptoms of LF are so varied ad nonspecific, therefore clinical diagnosis is often difficult; • Approximately 15%-20% of patients hospitalized for LF die from the illness; overall case-fatality rate is 1%; • Death rates are particularly high for women in the third trimester of pregnancy, and for fetuses, about 95% of which die in the uterus of infected pregnant mothers. • The need for early diagnosis!!!
What needs to be done to address the threat of LASSA FEVER!!! • Continually/further educating people in high-risk areas about ways to decrease rodent populations in their homes – this will aid in the control and prevention of Lassa fever; • Need to develop more rapid diagnostic tests and increasing the availability of the only known drug treatment – RIBAVIRIN. • Research is ongoing to develop a vaccine for Lassa fever.
SUMMARY OF ACTIONS • Case definition for Lassa Fever: • Suspected case: Illness with onset of fever and no response to usual causes of fever in the area, and at least one of the following signs: bloody diarrhoea, bleeding from gums, bleeding into skin, bleeding into eyes and urine; • Confirm case: A suspected case with laboratory confirmation (Positive IgM antibody or viral isolation), or epidemiologic link to confirmed cases or outbreak.
COMMON CLINICAL PRESENTATION • Major signs: • Confirmed contact with a patient with LF, • Abdominal bleeding (mouth, nose, rectum and/or vagina), • Oedema of the neck and/or face • Conjunctiva or sub-conjuctivahaemorrhage, • Jaundice; spontaneous abortion; deafness • Persistent hypotension • Elevated liver transaminases (SGOT/AST), 159IU/L
Clinical presentations contd • Minor signs: • General malaise, • Headache, • Retrosternal pain • Muscle or join pain • Cough, sore throat, • Abdominal pain, diarrhoea • Proteinuria, • Leucopoenia <4000 IU/L
MANAGEMENRT OF CASES • Suspected cases: • Anti-malarial, antibiotics, monitor temperature, look out for the signs listed above; • Confirmed cases: - Weigh patient, IV line, group and cross matching of blood, give oxygen if RR>20; • IV RIBAVIRIN: (loading dose: 33mg/kg; then day 1-4: 16mg/kg 6 hrly; then day 5-10: 8mg/kg 8 hrly) • If seizures – IV diazepam (with oxygen).
Precautions to take when treating cases: • NSAIDS are contraindicated due to risk of bleeding; • Avoid IM route of administration to avoid hematoma; • Use cotton wool to clean and dressed gently; • Avoid nasogastric tube, urinary catheter insertion as much as possible; • DO NOT remove old blood clot from previous bleeding sites • NEVER recap needles;
Precautions contd: • For pregnant patients, gentle vaginal examination is done only infrequently; • Patients experiencing seizures are given diazepam and put under oxygen concentration • Do not enter patient’s room or get in contact with a patient until you put on full personal protective equipment (PPE)
Poor prognostic indicators • Pregnant women • Bleeding cases • Tremors/seizures • Serum AST > 150 IU/ml • Late commencement of RIBAVIRIN (after 10th day of onset of illness).
THANK YOU //////////////////////////////////////////////////