Download
1 / 87
950 likes | 1.75k Views
Drug Eluting Versus Bare Metal Stents. Prof. Dr. Raouf Mahran ;MRCP Prof. of cardiovasc. Med National Heart Institute 2009. Historical back grounds. Evolution of PCI. 1977: Balloon Angioplasty (POBA) 1994: Bare Metal Stent (BMS) 2003: Drug Eluting Stent (DES).

E N D
Drug Eluting Versus Bare Metal Stents Prof. Dr. Raouf Mahran ;MRCP Prof. of cardiovasc. Med National Heart Institute 2009
Evolution of PCI 1977: Balloon Angioplasty (POBA) 1994: Bare Metal Stent (BMS) 2003: Drug Eluting Stent (DES)
PCI Procedural refinements: Stents Expandable metal mesh tubes that buttresses the dilated segment, limit restenosis. Drug eluting stents: further reduce cellular proliferation in response to the injury of dilatation.
What is a Drug-Eluting Stent (DES)? Example:Cordis’ Cypher™ Sirolimus-Eluting Coronary Stent Components • Stent Platform & Delivery System • Carrier(s) • Drug DHHS/FDA/CDRH
Binds tubulin Microtubular dynamics Multicellular Multifunctional TAXUS Technology Polymer Paclitaxel Platform • Uniformity • Durability • Biphasic Controlled Release Kinetics • Express™ Stent Tandem Architecture Flexibility • Maverick™ Balloon Deliverability
Drug-Eluting Stents The “HOLY GRAIL” of interventional cardiology is a stent with optimal deliverability and scaffolding which is impervious to intimal hyperplasia
Drug-Eluting Stents Clinical imperatives… • Reduced Restenosis - Efficacy • Goal = <10% restenosis frequency for all patient cohorts and all lesion subsets • Simulate normal wound healing with rapid endothelialization and minimal (? no) neointima formation • Absence of Pathobiologic Responses - Safety • No early or late thrombosis • No “edge” hyperproliferative effects • No late aneurysms, delayed “catch-up” (late restenosis), accelerated atherosclerosis
Drug-Eluting Stents Three Component System Stent design Drug-Eluting Stent Pharmacologic agent Drug carrier vehicle
Neointimal Hyperplasia (30%) Why DES??- Coz of Restenosis - Causes & Solution Causes Recoil & Negative Remodeling (70%) Solution • A stent to block recoil and remodeling • A therapeutic agent to prevent neointimal hyperplasia
Therapeutic Mechanisms of Action Growth Factors / Cytokines Receptor Smooth muscle cell • Activation FKBP Rapamycin and derivatives • Signal • Transduction TOR p27, Cyclins/Cdks Radiation Actinomycin D, (DNA) X S cell cycle G1 G2 G0 Paclitaxel, (microtubules) M Cell Division
Drug-Eluting Stents Stent Design… • Optimized geometry for homogeneous drug distribution (closed vs. open cell designs, inter-strut distances) • Circumferential stent-vessel wall contact (to insure drug delivery) - conformability • Enhanced radiopacity for precise placement (avoid overlap regions and inter-stent gaps) • Maintained side-branch access • Advanced deliverability to complex anatomies
Drug-Eluting Stents Drug Carrier Vehicle…requirements • Non-inflammatory and non-thrombogenic • Predictable drug elution kinetics (timing and dose) • Elastomeric without surface integrity changes (e.g. cracking, peeling) • No alteration of incorporated drug activity • No alteration of the structural and operational stent characteristics • Logistic factors – sterilization, stability, shelf-life, and expense
2mm } Top- coat } } 5mm 5mm { Sub- layer Stent COOK CORDIS GUIDANT PC coating 1mm + + + + + 1mm } } Nanoporous ceramic BiodivYsio Matrix LO Boston Scientific BiodivYsio Matrix HI JOMED Degradable polymer Degradable stent Degradable inlays SORIN CONOR-Medsystems Biosensor Igaki-Tamai Methods of Stent-Mediated Delivery
SIRIUS - Study Flow All Randomized Patients n = 1101 De-registered Control Bx VELOCITYTM (n=20) De-registered Sirolimus-eluting Bx VELOCITYTM (n=23) Sirolimus-eluting Bx VELOCITYTM n = 533 Control Bx VELOCITYTM n = 525 Angio FU at 8 Months = 84.7% Clinical FU at 9 Months = 95.8% Angio FU at 8 Months = 85.4% Clinical FU at 9 Months = 95.7%
The Realism of Drug Eluting Stents First FIM- Two Sites, 45 patients 0% Restenosis RAVEL Multicenter, Randomized 238 patients 0% Restenosis SIRIUS 400- Multicenter, Randomized 400 pts 9.2% Restenosis SIRIUS Final Results 1058 pts 8.9% Restenosis MACE at 24 Months 5/45=11.1% Than Than NOW
Current Indications for Drug-eluting Stents: • Why do we need DES ? • Which DES should we use ? • Indications for DES ?
Restenosis Elastic recoil: after balloon deflation, the large number of elastic fibers in the tunica media cause a mechanical collapse. Neointimal proliferation (NI): formation of an inner layer at the site of injury, composed of cells and ECM on the intimal surface Negative remodeling: constriction of the vessel by the formation of a fibrotic scar within the adventitia.
Intervention 2003 • Stents: the dominant strategy in interventional cardiology • Improved procedural safety • Predictable angiographic results • Better late outcomes (lower restenosis)
Current Indications for Drug-eluting Stents: • Why do we need DES ? • Which DES should we use ? • Indications for DES ?
100 randomised DES Studies in 49.993 Patients ABSOLUTE, ACTION, APPLAUSE, ASPECT, AVELLINO, BASKET, BBK, BRADES, CACTUS, CARDIA, CHINA-1, CHINA-2, CHREDIT, CORPAL, CORPAL-Bif-1, CORPAL-Bif-2, COSTAR-II, C-SIRIUS, Cypher/ BeStent, Cypher/Vision, DEDICATION-DES, DECODE, DELIVER-I, DESSERT, DEXA, DEXAMET, DIABETES, EAGLE, ELUTES, ENDEAVOR-II, ENDEAVOR-III, ENDEAVOR-IV, E-SIRIUS, ESTRADIOL, ETHOS-I, EUROSTAR-II, FUTURE- I, FUTURE-II, GENESIS, GENOUS-STEMI, HAAMU, HORIZONS-AMI, ISAR- DESIRE, ISAR-DIABETICS, ISAR-LM, ISAR-PEACE, ISAR-SMART-3, ISAR- TEST, ISAR-TEST-3, JUPITER-II, LABEM, LEADERS, LONG-DES-II, MISSION, NOBORI-I Phase 1, NOBORI-I Phase 2, NORDIC-Bif-I, NORDIC- Bif-II, PAINT, PASSION, PATENCY, PISA-LAD, PRISON-II, PROSIT, RAPPAC, RAVEL, RIGA-LM, RRISC, REALITY, RIBS-II, SCANDSTENT, SCORE, SCORPIUS, SESAMI, SES-SMART, SEVILLA, SIRIUS, SIRIUS-Bif, SIRTAX, SISR, SORT-OUT-II, SORT-OUT-III, SOS, SPIRIT-I, SPIRIT-II, SPIRIT-III, STEALTH-I, STRATEGY, SYNTAX, TAXI, TAXUS-I, TAXUS-II, TAXUS-IV, TAXUS-V, TAXUS-V-ISR, TAXUS-VI, TYPHOON, ZEST, ZOOMAX-I, ZOOMAX-II
1. High Evidence (primary clinical endpoint reached) Cypher Sirolimus Taxus (Cordis / J&J) (Boston Scientific) Paclitaxel Endeavor (Medtronic) Zotarolimus Xience V / Promus (Abbott / Boston Sc.) Everolimus Biomatrix (Biosensors/Krauth) Biolimus A9 • Medium Evidence (primary surrogate reached) Yukon (Translumina) Sirolimus Nobori (Terumo) Biolimus A9
Current Indications for Drug-eluting Stents: • Why do we need DES ? • Which DES should we use ? • Indications for DES ?
Should We Use Drug-Eluting Stents in All Patients and in All Lesions? NO Just Play it Smart
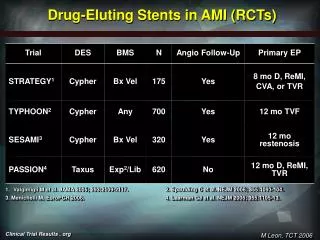
Indications Anticipated Approval • De-Novo Lesions • Length 15-30 mm • Vessel sizes 2.5-3.5 Not Approved (off label use) • Acute MI (Yes Recent data:Sirolimus), Acute Coronary Syndrome? • In-Stent Restenosis (ISAR 11 favours Sirolimus) • Bifurcations, long lesions>30 mm, small vessels< 2.5mm • SVG ?? • Multivessel (Syntax approves LMS+1,2vessels).