Download
1 / 51
570 likes | 1.77k Views
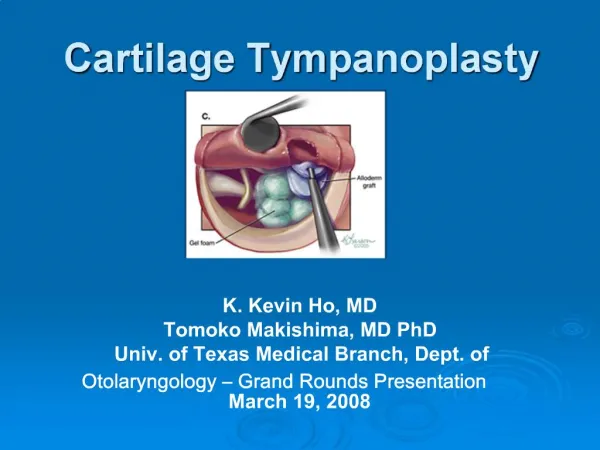
Principles of tympanoplasty. By : Dr. Supreet Singh Nayyar, AFMC For more presentations , visit www.nayyarENT.com. Layout. History & evolution of middle ear surgery Definition of tympanoplasty The transformer mechanism in health and disease Functional considerations of tympanoplasty

E N D
Principles of tympanoplasty By : Dr. Supreet Singh Nayyar, AFMC For more presentations , visit www.nayyarENT.com www.nayyarENT.com
Layout History & evolution of middle ear surgery Definition of tympanoplasty The transformer mechanism in health and disease Functional considerations of tympanoplasty Classification Principles of tympanoplasty surgery Basics of ossiculoplasty Reporting protocols Pediatric tympanoplasty Recent advances www.nayyarENT.com
Evolution of Middle Ear Surgery Era of Experimentation 19th century Era of Opposition Late 19th & early 20th century Era of Revival 1920’s Era of Reorientation 1940’s - 1960’s Era of Modernity From then on..... www.nayyarENT.com
Acoustic transformer mechanism Ossicular coupling Hydraulic lever Ossicular lever Catenary lever Acoustic coupling www.nayyarENT.com
Transformer in Diseased State Effect on Ossicular coupling Ossicular Discontinuity Ossicular Fixity Effect on Acoustic coupling Loss of Round Window shielding Effect of Stapes, Cochlear & RW Impedance Middle ear aeration / fluid www.nayyarENT.com
Definition of Tympanoplasty “ Procedure to eradicate disease in the middle ear & to reconstruct the hearing mechanism with/without TM (tympanic membrane) grafting ”* * 1965- American Academy of Ophthalmology & Otolaryngology Subcommittee on Conservation of Hearing www.nayyarENT.com
Goals of Surgery To establish intact tympanic membrane Eradication of middle ear disease & create an air containing middle ear space Restore hearing by building a secure connection between the tympanic membrane & cochlea www.nayyarENT.com
Techniques Minimalistic techniques Cauterization & fat plug Cauterization with trichloroacetic acid Sealed tympanostomy tubes Formal Tympanoplasty www.nayyarENT.com
Classification of Tympanoplasty 1956- Wullstein Type 1 Type 2 Type 3 Type 4 Type 5 www.nayyarENT.com
Classification of Tympanoplasty • Mirko Tos • 1 - Intact chain • 2 – Short columella • 3 – Long columella • 4 - Sound protection • 5A - Fenestration of LSCC • 5B - Platinectomy www.nayyarENT.com
Indications Conductive hearing loss due to TM perforation or ossicular dysfunction Chronic or recurrent otitis media Progressive hearing loss due to chronic middle ear pathology Perforation or hearing loss persistent for more than three months due to trauma, infection or surgery Inability to bathe or participate in water sport activities (ArunGadre, Christopher Muller, University of Texas Branch, Texas) www.nayyarENT.com
Contraindications (Glasscock 1976 / Shambaug) Absolute Uncontrolled cholesteatoma Malignant tumors Unusual infections Intracranial complications Relative Eustachian tube dysfunction / OME in other ear Dead ear Only hearing ear Elderly patient Very young children Repeated failures Uncooperative patients www.nayyarENT.com
Preoperative Evaluation Extent & location of perforation Ossicular status Counseling Nature of disease Treatment options Outcomes of surgical options Post op morbidity – restriction of water activities, hearing deterioration www.nayyarENT.com
Approach Transcanal Posterior moderate sized perforations Favorable EAC anatomy Endaural Visualisation of annulus & ant sulcus is difficult Limited atticotomy Postaural All perforation sizes Better angle of visualisation Second look ossiculoplasty www.nayyarENT.com
Graft Placement Lateral / Overlay Medial / Underlay Over-Underlay www.nayyarENT.com
Contd… Overlay Adv Exposure of anterior meatal recess High take up rate Middle ear volume not reduced Disadv Precision is required Long healing time Blunting / lateralization Underlay Adv Less blunting or lateralization High graft take up in experienced hands Simpler technique/less time consuming Disadv Limited visualisation of ant meatal recess Less suitable for large ant perf Difficult in small EAC with per meatal approach Reduction in ME space www.nayyarENT.com
Results – Underlay / Overlay Technique Review of Underlay versus Overlay tech * Re-perf rate - 36% Overlay, 14% Underlay Hearing improvement – 62% Underlay, 27% Overlay Complication rate less in Underlay Review of Overlay tech** Graft uptake 97% - Temp fascia, 84% -Canal skin Rate of Ant blunting & Lateralization 1.3% AB gap within 10 dB – 80% Review of Underlay versus Overlay tech*** Graft uptake - 89% Underlay, 96% Overlay Hearing improvement – 85% Underlay, 80% Overlay Complications – 7.8% Underlay, 9% Overlay * Doyle et al(1972), ** Sheehy et al, *** Rizer (1997) www.nayyarENT.com
Graft Materials Autografts Skin Canal skin Pedicled Free Heterotopic skin graft Periosteum Vein Temporalis fascia Fatty tissue Tragal perichondrium & cartilage Subcutaneous tissue www.nayyarENT.com
Graft Materials Allografts Historical Amnion Cornea Duramater Peritoneum Pericardium Aorta valves Ear drum Lyophiliseddura Cartilage Fascia Risk of HIV, Hepatitis B, Creutzfeldt Jacob disease Xenografts Historical Bovine Periostem Drum Jugular vein www.nayyarENT.com
Reasons for Graft failure Technical/surgeon errors Infectious complications Poor tubal function Patient factors www.nayyarENT.com
Ossicular status Austin / Kartush Classification www.nayyarENT.com
Autografts Bone Cartilage Materials used in Ossiculoplasty www.nayyarENT.com Conchal /Tragal Cartilage • Adv • Immediate availability • Biocompatibility • Low cost • Low extrusion rate • Disadv • Disease recurrence • Fixation to adjacent structures • Skill & time to shape
Homografts www.nayyarENT.com Irradiated Ossicles En Bloc TM with attached Ossicles Risk of disease transmission
Allografts www.nayyarENT.com • Biocompatible • 1960’s – Polyethylene tubing, Teflon, Proplast • 1970’s – HDPS (Plastipore), Thermal fused HDPS (Polycel) • Silastic, Stainless steel, Titanium • Bioinert • Al 2O3 Ceramic (Germany & Japan in 1970’s) • Bioactive • Bioactive glass – Bioglass, Ceravital (1970’s) • CaPO4 Ceramic - Hydroxyapatite
Configurations of Allografts www.nayyarENT.com Total Ossicular Replacement Prosthesis (TORP) Partial Ossicular Replacement Prosthesis (PORP) Prosthesis for ossicular discontinuity restricted to IS joint Combined forms - Hydroxyapatite platform with Plastipore shaft
Different Types of Prosthesis www.nayyarENT.com
Ossiculoplasty • Choice of prosthesis / placement • Ossicular status • Med – lat distance / vertical position • Retracted umbo – severing of tensor tympani tendon www.nayyarENT.com
Surgical Techniques in case of ossicular fixation Tympanosclerosis Disease restricted to attic Disease restricted to stapes Combined attic & stapedial disease Acquired bony fixation Removal of fixation with intact chain Removal of incus/malleus head with interposition of allograft/autograft www.nayyarENT.com
Surgical Techniques for ossicular discontinuity Ossicular status Lenticular process missing Tip of Incus missing Long process of Incus missing Stapes superstructure +/- Malleus handle +/- www.nayyarENT.com
Configurations of Prosthesis www.nayyarENT.com
Factors affecting outcomes of ossiculoplasty Intrinsic factors Status of ossicular chain – mobility Severity of disease Eustachian tube function Adequate control of allergy www.nayyarENT.com
Contd… www.nayyarENT.com • Extrinsic Factors • Surgical technique • Design of prosthesis • Composition of prosthesis
Advantages of Titanium Prosthesis www.nayyarENT.com • Low wt (<4mg), high rigidity • Open head plate design- better visualisation during placement • Medial end has claw like design- better fit on stapes head • Unlike hydroxyapatite they are not top heavy, stay upright
Poor Eustachian Tube Function www.nayyarENT.com • Cartilage Tympanoplasty • Prevent recurrence of retraction pockets • May reduce extrusion rates • Mainly with Temporalis Fascia grafts • Posterosuperior TM/post Pars Flaccida* • Entire TM** • Composite cartilage peri- chondrium graft • Cartilage Palisade technique*** ( * Poe & Gadre :1993; ** Dornhoffer :1997; *** Heerman )
Poor ET Function (contd…) www.nayyarENT.com • Tympanostomy • Rarely at the time of TM grafting • Maybe during follow up if effusion or retraction develops
Middle Ear Stents www.nayyarENT.com • Teflon / Silicone pieces • Silastic sheet • Biodegradable materials • Gelfoam • Gelfilm
Reporting protocols “ Fiction & fact need untangling, otherwise, surgeons are little better than gossips ” :Gordon Smyth
Reporting Protocols www.nayyarENT.com • Tympanoplasty Reporting Protocol based on AB gap (Kartush) AB gapResult 0 – 10 dB Excellent 10 – 20 dB Good 20 – 30 dB Fair >30 dB Poor
Reporting Protocols www.nayyarENT.com • For Disease* • Type & location of perforation • Ossicular status • Status of mucosa • Status of eustachian tube • For Results* • Control of pathology • Anatomic status • Improvement in hearing • Post-op complications (*American Academy of Ophthalmology & Otolaryngology Subcommittee on Conservation of Hearing)
Middle ear risk index MERI 0 Normal MERI 1-3 Mild disease MERI 4-6 Moderate disease MERI 7-12 Severe disease www.nayyarENT.com
Tympanoplasty Reporting Protocol www.nayyarENT.com
Reporting Protocols (contd…) www.nayyarENT.com • Pure Tone Averages • Frequencies : 500 Hz, 1 KHz, 2 KHz, 3 KHz * • Most commonly affected frequencies by Conductive Hearing Loss • Glasgow Benefit Plot ** • * Recommendation of The American Academy of Otolaryngology – Head & Neck Surgery • ** Browning et al : Glasgow Benefit Plot : A new method for reporting results of middle ear surgery; 1991, Laryngoscope101 : 180-185
Hearing Evaluation • Belfast Rule Of Thumb * • Post operative air conduction mean threshold over speech frequencies <30 dB • Inter aural air conduction mean threshold <15dB *Smyth & Peterson, 1985 www.nayyarENT.com
Paediatric Tympanoplasty www.nayyarENT.com • Controversy - Mgt of pts with TM perforation(+/-otorrhea) • Factors affecting decision of surgery • Poor tubal function( perforation acts as natural grommet) • Frequent episodes of URTI • Negative middle ear pressure in contralateral ear
Recent Advances – Uses of Laser • Extraction of ankylosed transposed ossicles in revision cases • Potassium Titanyl Phosphate LASER for amputation of malleus & incus & at the same time maintaining chain integrity * • LASER Soldering tech ( Solid State Diode LASER )** * Nishizaki K et al; Nov 2001 vol 22 issue 6 Pg 424-427, Head & Neck Medicine & Surgery ** Study on cadaveric human temporal bones www.nayyarENT.com
Conclusion www.nayyarENT.com Rich history Antibiotics & binocular microscope major role brought turnaround Better & better results with tympanoplasty Newer materials for ossiculoplasty Scope of further research e.g. in area of cartilage & pediatric tympanoplasty
References www.nayyarENT.com Text book of Otolaryngology – Head & Neck Surgery : Charles W Cummings, 4thed , vol 4, 3058 – 74 Manual of Middle Ear Surgery : MirkoTos, vol 1 The Otolaryngologic Clinics of North America : Aug 1994; Ossiculoplasty, vol 27, No 4 Surgery of the Ear : Glasscock – Shambough, 5thed Scott Brown otolaryngology 7th edition Internet Journal articles