Download
1 / 11
110 likes | 447 Views
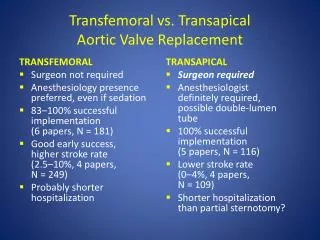
Dilatation of the remaining aorta following aortic valve or root replacement in patients with bicuspid aortic valve. Gopal K. R. Soppa, Nada R. Abdulkareem, Siôn Jones , Oswaldo Valencia, Aiman Alassar, Marjan Jahangiri Department of Cardiac Surgery, St George’s Hospital, University of London

E N D
Dilatation of the remaining aorta following aortic valve or root replacement in patients with bicuspid aortic valve Gopal K. R. Soppa, Nada R. Abdulkareem, Siôn Jones,Oswaldo Valencia, Aiman Alassar, Marjan Jahangiri Department of Cardiac Surgery, St George’s Hospital, University of London Declaration of interest None
Background Bicuspid aortic valve (BAV) is the commonest cardiac defect, 1-2% 40% association with aortic aneurysm Hemodynamic turbulence theory: Uneven current present (different jet patterns) More in aortic root and arch More in convexity or aorta Intrinsic aortic wall defect theory: BAV aortas have less fibrillin-1, independent of valve function Cystic medial necrosis is similar in BAV and in Marfan syndrome Aorta continues to dilate post AVR Aortic aneurysm exist even with normally functioning BAV Combination Evangelista et al; Curr Cardio Rep 2011 McKellar et al; Am J Cardio 2010
Background-Cont. Nine times risk of aortic dissection Complications occurring a decade younger than the normal population The natural history and management of dilatation of the aorta in patients with BAV following aortic valve replacement (AVR) or aortic root replacement (ARR) remain controversial Svensson et al; JTCVS 2011 Elefteriades et al; JTCVS 2010
Aim • To identify dilatation of the remaining aorta following AVR or ARR in patients with BAV compared to patients with tricuspid aortic valve (TAV) • This can serve as a guide to perform prophylactic ARR in BAV patients
Methods • Retrospective analysis, 2002-2009 • n=395, BAV=192 , TAV=203 , AVR and/or ARR • Serial echocardiograms were studied, median follow-up of 3.8 years (1.2-6.8 years) • Preoperative, postoperative • 6 months • 1, 3, 5 years • Standard aortic measurements were taken (annulus, STJ, ascending aorta, aortic arch) • ARR patients had serial CT scans • Patients with other connective tissue disorders were excluded • Ascending aorta diameter ≥4.5cm was regarded aneurysmal
n= 395 Referred for AVR or ARR BAV + Normal Aorta n=143 (36%) BAV + Dilated Aorta n=49 (12%) TAV + Normal Aorta n=129 (33%) TAV + Dilated Aorta n=74 (19%) Patient Classification
Results-1 Aortic Sinus of Valsalva Dimensions *** ***
Results-2 Ascending Aorta Dimensions ***
Results-3 Aortic Arch Dimensions
Conclusions • No significant dilatation of the aorta was observed following AVR or ARR in patients with BAV compared with TAV up to 5 years following surgery • This supports intervention only with ascending aorta ≥4.5cm in BAV patients with concomitant valvular disease