Download
1 / 1
10 likes | 181 Views
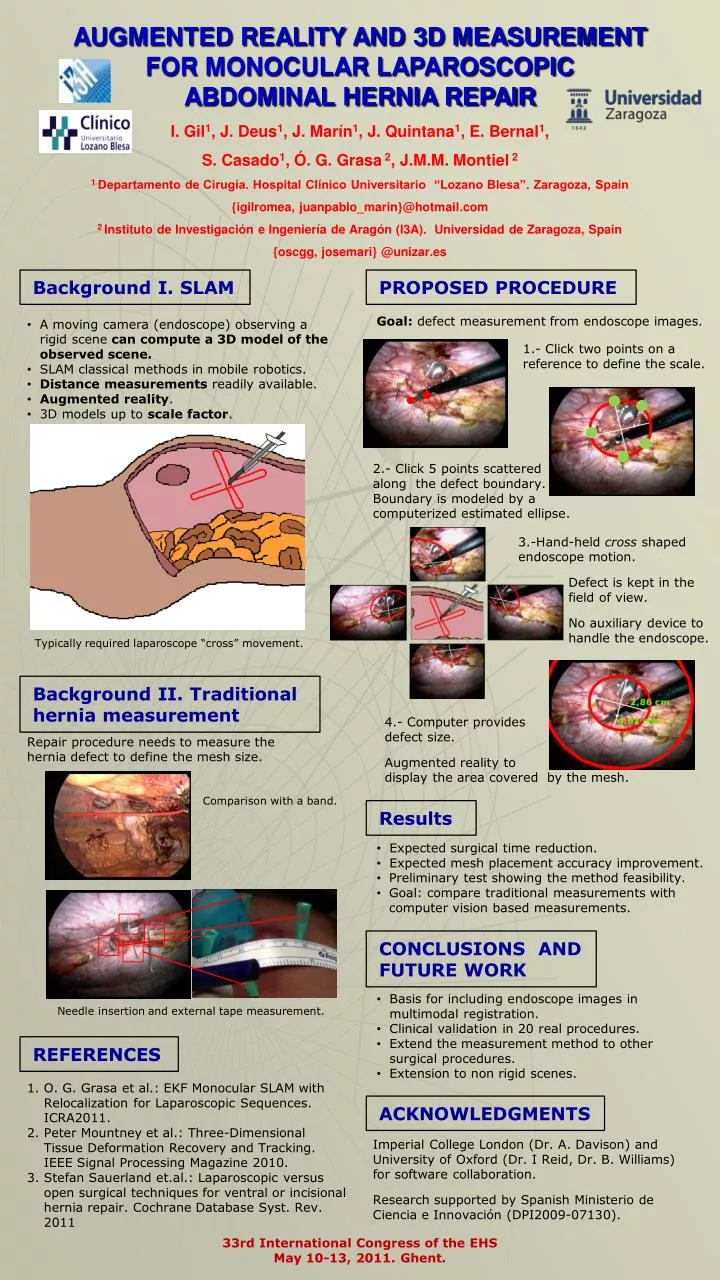
AUGMENTED REALITY AND 3D MEASUREMENT FOR MONOCULAR LAPAROSCOPIC ABDOMINAL HERNIA REPAIR. I. Gil 1 , J. Deus 1 , J. Marín 1 , J. Quintana 1 , E. Bernal 1 , S. Casado 1 , Ó. G. Grasa 2 , J.M.M. Montiel 2

E N D
AUGMENTED REALITY AND 3D MEASUREMENT FOR MONOCULAR LAPAROSCOPIC ABDOMINAL HERNIA REPAIR I. Gil1, J. Deus1, J. Marín1, J. Quintana1, E. Bernal1, S. Casado1, Ó. G. Grasa 2, J.M.M. Montiel 2 1 Departamento de Cirugía. Hospital Clínico Universitario “Lozano Blesa”. Zaragoza, Spain {igilromea, juanpablo_marin}@hotmail.com 2 Instituto de Investigación e Ingeniería de Aragón (I3A). Universidad de Zaragoza, Spain {oscgg, josemari} @unizar.es Background I. SLAM PROPOSED PROCEDURE Goal: defect measurement from endoscope images. • A moving camera (endoscope) observing a rigid scene can compute a 3D model of the observed scene. • SLAM classical methods in mobile robotics. • Distance measurements readily available. • Augmented reality. • 3D models up to scale factor. 1.- Click two points on a reference to define the scale. 2.- Click 5 points scattered along the defect boundary. Boundary is modeled by a computerized estimated ellipse. 3.-Hand-held cross shaped endoscope motion. Defect is kept in the field of view. No auxiliary device to handle the endoscope. Typically required laparoscope “cross” movement. Background II. Traditional hernia measurement 4.- Computer provides defect size. Augmented reality to display the area covered by the mesh. Repair procedure needs to measure the hernia defect to define the mesh size. Comparison with a band. Results • Expected surgical time reduction. • Expected mesh placement accuracy improvement. • Preliminary test showing the method feasibility. • Goal: compare traditional measurements with computer vision based measurements. CONCLUSIONS AND FUTURE WORK • Basis for including endoscope images in multimodal registration. • Clinical validation in 20 real procedures. • Extend the measurement method to other surgical procedures. • Extension to non rigid scenes. Needle insertion and external tape measurement. REFERENCES O. G. Grasa et al.: EKF Monocular SLAM with Relocalization for Laparoscopic Sequences. ICRA2011. Peter Mountney et al.: Three-Dimensional Tissue Deformation Recovery and Tracking. IEEE Signal Processing Magazine 2010. Stefan Sauerland et.al.: Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. Cochrane Database Syst. Rev. 2011 ACKNOWLEDGMENTS • Imperial College London (Dr. A. Davison) and University of Oxford (Dr. I Reid, Dr. B. Williams) for software collaboration. • Research supported by Spanish Ministerio de Ciencia e Innovación (DPI2009-07130). 33rd International Congress of the EHS May 10-13, 2011. Ghent.