Download
1 / 1
10 likes | 119 Views
Quality Improvement &Cost Savings through Patient Centered Medical Homes. LOGO. LOGO.

E N D
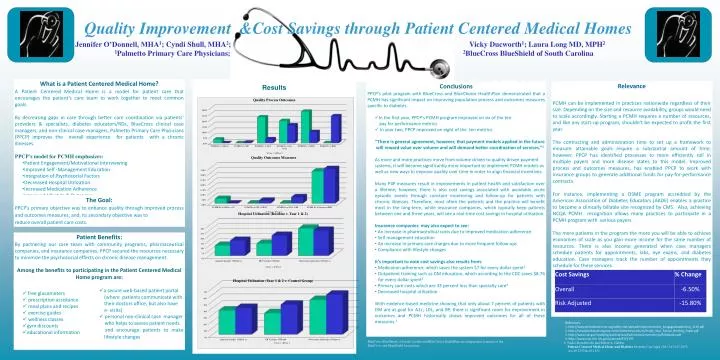
Quality Improvement &Cost Savings through Patient Centered Medical Homes LOGO LOGO Jennifer O’Donnell, MHA1; Cyndi Shull, MHA2; Vicky Ducworth1; Laura Long MD, MPH2 1Palmetto Primary Care Physicians; 2BlueCross BlueShield of South Carolina • What is a Patient Centered Medical Home? • A Patient Centered Medical Home is a model for patient care that encourages the patient’s care team to work together to meet common goals. • By decreasing gaps in care through better care coordination via patients’ providers & specialists, diabetes educators/RDs, BlueCross clinical case managers, and non-clinical case managers, Palmetto Primary Care Physicians (PPCP) improves the overall experience for patients with a chronic illnesses. • PPCP’s model for PCMH emphasizes: • Patient Engagement/Motivational Interviewing • Improved Self -Management Education • Integration of Psychosocial Factors • Decreased Hospital Utilization • Increased Medication Adherence • Improved Lifestyle & Outcomes Results • Conclusions • PPCP’s pilot program with BlueCross and BlueChoice HealthPlan demonstrated that a PCMH has significant impact on improving population process and outcomes measures specific to diabetes. • In the first year, PPCP’s PCMH program improved on six of the ten • pay for performance metrics. • In year two, PPCP improved on eight of the ten metrics. • “There is general agreement, however, that payment models applied in the future will reward value over volume and will demand better coordination of services.”1 • As more and more practices move from volume driven to quality driven payment systems, it will become significantly more important to implement PCMH models as well as new ways to improve quality over time in order to align financial incentives. • Many P4P measures result in improvements in patient health and satisfaction over a lifetime; however, there is also cost savings associated with avoidable acute episodic events through constant monitoring and follow-up for patients with chronic illnesses. Therefore, most often the patients and the practice will benefit most in the long-term, while insurance companies, which typically keep patients between one and three years, will see a real-time cost savings in hospital utilization. • Insurance companies may also expect to see: • An increase in pharmaceutical costs due to improved medication adherence • Self management education • An increase in primary care charges due to more frequent follow-ups • Compliance with lifestyle changes • It’s important to note cost savings also results from: • Medication adherence, which saves the system $7 for every dollar spent2 • Outpatient training such as DM education, which according to the CDC saves $8.76 • for every dollar spent3 • Primary care costs which are 33 percent less than specialty care4 • Decreased hospital utilization • With evidence-based medicine showing that only about 7 percent of patients with DM are at goal for A1c, LDL, and BP, there is significant room for improvement in outcomes and PCMH historically shows improved outcomes for all of these measures.5 Relevance PCMH can be implemented in practices nationwide regardless of their size. Depending on the size and resource availability, groups would need to scale accordingly. Starting a PCMH requires a number of resources, and like any start-up program, shouldn’t be expected to profit the first year. The contracting and administration time to set up a framework to measure attainable goals require a substantial amount of time; however, PPCP has identified processes to more efficiently roll in multiple payers and more disease states to this model. Improved process and outcomes measures, has enabled PPCP to work with insurance groups to generate additional funds for pay-for-performance contracts. For instance, implementing a DSME program accredited by the American Association of Diabetes Educators (AADE) enables a practice to become a clinically billable site recognized by CMS. Also, achieving NCQA PCMH recognition allows many practices to participate in a PCMH program with various payers. The more patients in the program the more you will be able to achieve economies of scale as you gain more income for the same number of resources. There is also income generated when case managers schedule patients for appointments, labs, eye exams, and diabetes education. Case managers track the number of appointments they schedule for these services. The Goal: PPCP’s primary objective was to enhance quality through improved process and outcomes measures; and, its secondary objective was to reduce overall patient care costs. Patient Benefits: By partnering our care team with community programs, pharmaceutical companies, and insurance companies, PPCP secured the resources necessary to minimize the psychosocial effects on chronic disease management. Among the benefits to participating in the Patient Centered Medical Home program are: • free glucometers • prescription assistance • meal plans and recipes • exercise guides • wellness classes • gym discounts • educational information • a secure web-based patient portal • (where patients communicate with • their doctors office, but also have • e- visits) • personal non-clinical case manager • who helps to assess patient needs. • and encourage patients to make lifestyle changes • References • 1. http://www.qhmedicalhome.org/safety-net/upload/Implementation_EnagagedLeadership_1110.pdf • 2. http://scriptyourfuture.org/wp-content/themes/cons/m/Script_Your_Future_Briefing_Paper.pdf • 3. http://www.cdc.gov/nccdphp/publications/factsheets/prevention/pdf/diabetes.pdf • 4. http://www.ncbi.nlm.nih.gov/pubmed/9722797 • 5. Trajko Bojadzievski and Robert A. Gabbay • Patient-Centered Medical Home and Diabetes Diabetes Care April 2011 34:1047-1053; • doi:10.2337/dc10-1671 BlueCross BlueShield of South Carolina and BlueChoice HealthPlan are independent licensees of the BlueCross and BlueShield Association






















