Download
1 / 29
310 likes | 838 Views
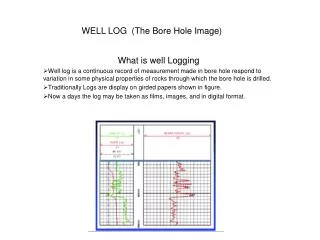
Macular Hole F.Fazel:MD. Pathophysiology of MH. Trauma Laser treatment Cystoid macular edema Inflammation Retinal vascular disease Retinal detachment Age-related primary idiopathic. Idiopathic MH. Seven decade Predominantly female(67%-91%) Younger age in myopes 1%-25% bilatera.

E N D
Pathophysiologyof MH • Trauma • Laser treatment • Cystoid macular edema • Inflammation • Retinal vascular disease • Retinal detachment • Age-related primary idiopathic
Idiopathic MH • Seven decade • Predominantly female(67%-91%) • Younger age in myopes • 1%-25% bilatera
Pathophysiology • Anteroposterior transvitreal traction????... • Tangential traction of cortical vitreous
Staging 1:impendiing MH(foveal &foveolar detached) 2:small fullthicknes MH)<400M) 3:fullthickness MH(>400M) 4:Complete PVD
Signs & symptomsstage 1 • Mild Central visual loss &metamorphopsia • Loss of foveal depression • Yellow spot or yellow ring • 50% resolved spontaneously • 50% progress to stage 2
Signs & sympomsstage 2-3 • Full thikness hole • Vision loss • Annular neurosensory detachment • Absolute scotoma((watzke-allen sign)
Sign & symptomsstage4 • Complete PVD (weiss ring)
Fluorescein Angiography • Circular transmission defect(stage 2-3-4) • Loss of xanthophyll & RPE atrophy
OCT • IS GOLD STANDARD IN DIAGNOSIS AND STAGING
Management • Stage 1:fallow up • Stage 2-4:vitrectomy +gas injection(90%-100% hole closure)