Download
1 / 32
320 likes | 336 Views
This population-based study examines the incidence, treatment patterns, and survival trends of Kaposi sarcoma in the Netherlands, highlighting its role as an indicator disease for HIV prevalence.

E N D
Kaposi sarcoma as indicator disease for HIV prevalence in the Netherlands A population-based study 12th of June 2019 | Vincent Ho | Harm Buisman | Jan Maarten van der Zwan
Historical perspective • Moritz Kaposi (1837–1902) • 1872: The disease leads to death, and it does sowithin a short period of two to three years...The disease must, from our present experience,be considered from the onset not only asincurable but also as deadly. Source: www.zsidokivalosagok.hu
Presentation • ‘classic’ form • elderly men; • skin lesions of lower extremities; • rarely nodal involvement; • indolent period 10–15 years; • systemic lesions or lymphoreticularmalignancies in late phase • African (‘endemic’) form • childhood form • transplant-associated form DePond, 2019
Presentation II • AIDS epidemic: ‘HIV-associated’ form • 1980s: significant proportions of homosexual men with AIDS(San Francisco: 40%; Vancouver: 56% among those with >20 partners) • multicentric, more aggressive behavior • disseminations involving mucosal tissues, progress to visceral organs • 1996: Kaposi sarcoma caused by human herpesvirus 8 (HHV8) • 1990s: stark decline in incidence with highly active antiretroviral therapy (US: 50% reduction with triple antiretroviral therapy) Curtiss, 2016; Jones, 2000
The Netherlands II • inhabitants: 17.3 million (2019) • total area: 41,500 sqkilometres (16,000 sq mi) • hospitals: 80 (approx)
Netherlands Cancer Registry • since: national data since 1989 (regionalfrom 1955) • coverage: >95% • incidence: >115.000 cases per year • database: >2 million cases • data collection, analysis and reporting:Netherlands ComprehensiveCancer Organization (IKNL)
Netherlands Cancer Registry II pathology laboratories NCR hospital discharge other databases
Netherlands Cancer Registry III • basic data • demographics (birth date, sex, postal code) • tumor characteristics (topography, morphology) • information on diagnosis • information on treatment (type, hospital) • information on follow-up (includingvital status) • additional data (tumor specific) • e.g. molecular markers, complications, pathological review(depending on tumor type)
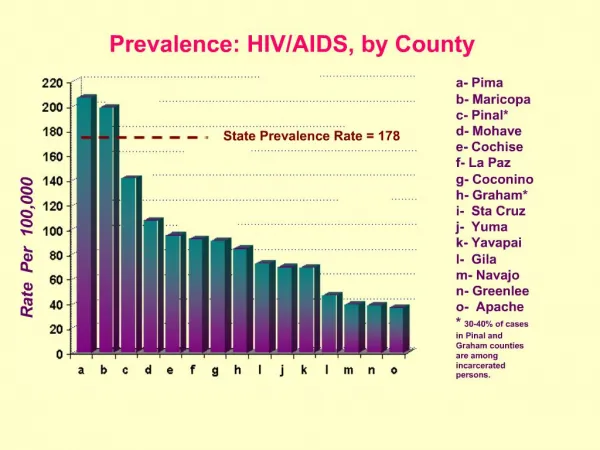
Methods • case selection • primary Kaposi sarcoma (M9140), histologicallyconfirmed • diagnosis in a Dutch hospital, 1989–2018 • residency in the Netherlands • incidence • byregion; based on postal code(definedforstatistical purposes, as used by Statistics Netherlands) • comparisonwith HIV-prevalence, byregion • treatment patterns • survival trends • age-standardized net survival
HIV Monitoring • 2017
Conclusions • Incidence of Kaposi sarcoma has been predominantly centered around the nation’s capital area of Amsterdam, mirroring reported figures on HIV prevalence • Survival of Kaposi sarcoma patients improved considerably over time • In general, Kaposi sarcoma may be conceived as indicator disease for HIV prevalence
Acknowledgements • Harm Buisman • Jan Maarten van der Zwan • team ‘Rare cancers’ • Annemiek Kwast • Ria de Peuter • Loes Verboord • Karin Fonken • Ria Jansen • Thekla Bluemink • Marlon Tonis