Download
1 / 23
230 likes | 333 Views
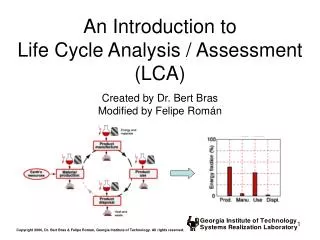
FATE: Family Assessment of Treatment at End-of-life. David J Casarett MD MA CHERP, Philadelphia VAMC Division of Geriatrics University of Pennsylvania. VA Mission: To Honor Veterans’ Preferences for Care at the End of Life.

E N D
FATE: Family Assessment of Treatment at End-of-life David J Casarett MD MA CHERP, Philadelphia VAMC Division of Geriatrics University of Pennsylvania
VA Mission: To Honor Veterans’ Preferences for Care at the End of Life "VA must offer to provide or purchase hospice & palliative care that VA determines an enrolled veteran needs." 38 CFR 17.36 and 17.38
How well are we doing? • Data are needed: • To identify problems • To distinguish high- vs. low-performing facilities • To guide improvement efforts • To shape policy related to: • Funding • Workforce • Health care systems organization
Opportunity to translate data into policy Opportunity for a public health approach/population-based Data-rich health care system and Electronic Medical Record Quality measurement opportunities in VHA
Data availability sets the VA apart: Potential for nationwide quality measurement • Structures of care • Consult services • HVPs • Inpatient units • Processes of care • Consults • Referrals to hospice • Outcomes (provide answers to key policy-relevant questions) • Do palliative care consults improve care? • Does home hospice improve care?
Background • HSRD-funded instrument development project • Multisite • 5 sites in initial phase (current) • 15 sites in feasibility test • Preliminary version approved by Office of Management and Budget as a quality tool (10/06) • Planned for review as a Type III (mandatory) Directors performance measure
Approach • Afterdeath telephone interview of families • Enrolled veterans who had at least one healthcare contact with the VA in the last month of life • Inpatient, outpatient, and NHCU deaths • Eligibility • National death bulletin notifications • Chart review • Letter to families • Telephone call (approximately 2 months after death)
Epidemiology of the veteran population (2005) • ~24,000,000 living veterans • ~687,000 projected veteran deaths (2005-2006) • ~100,000 enrolled deaths • ~29,000 inpatient deaths VA is responsible VA is accountable Only the VA is accountable http://www.va.gov/vetdata/demographics/index.htm
Sites (Phase I) • Philadelphia • Birmingham • West Los Angeles • Louisville • Lebanon
Domains • Well-being and dignity (5 items) • Communication (4 items) • Care consistent with preferences (2 items) • Symptom management (4 items) • Care around the time of death (5 items) • Emotional/spiritual support (4 items) • VA services (3 items) • VA death benefits (3 items) • Admitted to facility of choice (1 item)
Reporting • Anonymous (self-identified only) • Domain scores and rankings • Future: case-mix adjusted • www.caringforveterans.org
Do palliative care consults improve care? Does home hospice improve care? Is home hospice better than inpatient palliative care? Value to the VA: Examples of 3 policy-relevant questions
Yes: 86% vs. 64% (p<0.001)* *Adjusted for age ethnicity, income, diagnosis (cancer vs. non-cancer), and site. Value to the VA: Do PC consults improve care? (FATE score, n=309)
Maybe: 89% vs. 85% (not significant)* BUT: Significant interaction by site (e.g. hospices in some cities have a greater effect than in others). *Adjusted for age, ethnicity, income, diagnosis (cancer vs. non-cancer) and LOS. Value to the VA: Does hospice improve care for deaths at home? (FATE score, n=143)
All hospices are not equal • Died at home with hospice: • Range across sites (means): 43-78 (P=0.010) • Small variation in VA service scores • Larger variation in VA death benefits • Large variation in communication, care around the time of death, and symptoms
No place like home? • Died at home with hospice: • FATE score mean 67 (IQ range 45-76) • Died in a VA hospital with palliative care: • FATE score mean 76 (IQ range 64-82) (P=0.014)
Preliminary results: summary • Inpatient PC improves care • Home hospice probably improves care • There is substantial variation among hospice programs • Inpatient PC may be as good as home hospice care
Next steps • Approval for QI use • Approval as a national quality measure • Rollout nationally • Central administration? • Central data collection • Routine reporting and integration into VISN quality initiatives
FATE collaborators and supporters: Ken Rosenfeld MD Christine Ritchie MD MPH Scott Shreve MD Christian Furman MD Amos Bailey MD Tom Edes MD Diane Jones MSW VA RCD 00008-01 and ARCDA VA HSRD IIR 03-128-2 VA CPP #217 VA CSP #476 Center for Health Equity Research and Promotion R01 CA109540-01 Paul Beeson Physician Scholars Award NIH K01 AI 01739-01 Hartford Foundation VistaCare Foundation Commonwealth Fund Greenwall Foundation Collaborators Support
Questions: • How to integrate with FEHC? • How could these data be useful to hospices? • How could hospice partner with VA facilities to help them improve their FATE scores?