Download
1 / 39
690 likes | 1.46k Views
Hairy Cell Leukemia HCL. Hairy cell leukemia is a chronic Lymphoprolifrative disorder. in 1952 was recognized. Leukemic reticuloendotheliosis. Lymphoid myelofibrosis. Reticulum cell leukemia. HCL Neoblastic B Lymphocyte. carry surface immunoglobulins of only one

E N D
Hairy cell leukemia is a chronic Lymphoprolifrative disorder. in 1952 was recognized. Leukemic reticuloendotheliosis. Lymphoid myelofibrosis. Reticulum cell leukemia.
HCL Neoblastic B Lymphocyte. carry surface immunoglobulins of only one light chain type Often isotype is of Gama class or Multiple heavy chain. H.cell express receptors for Fc portion of IgG. IgM HCL reactivity with antibodies to CD19 .CD20, CD22 , CD25 , CD103 and MLA-DR. PCA-1 is detected in HC & Plasma cell. ( CD11c, CD25 and CD103 )
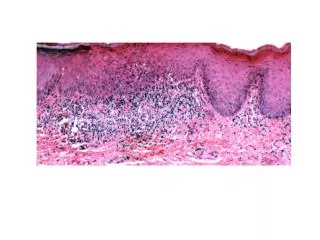
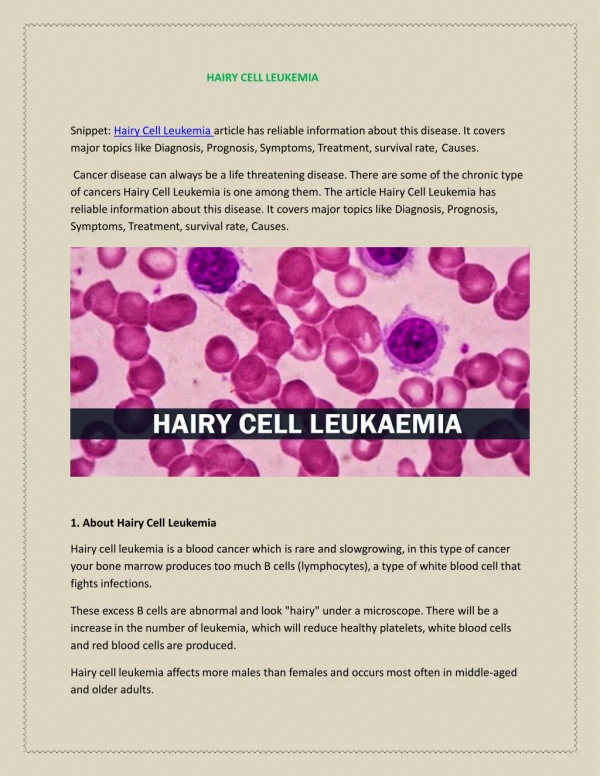
The hairy cells are 10 to 15 mm in diameter with pale blue cytoplasm and a nucleus with a loose chromatin structure and one or two indistinct nucleoli.
Hairy Cell Leukemia In PBS Pancytopenia Lymphocytosis Hairy cell Infection Middle age Male / female
Symptomatology: Patients have fatigue due to anemia, fever, weight loss, and/or abdominal discomfort. Sometimes the disease is diagnosed when patients have infection secondary to granulocytopenia or monocytopenia. The only consistent physical findings are slight to marked splenomegaly (75 to 80% of cases)
Bone marrow aspiration is usually inadequate owing to increased reticulin, collagen, and fibrin deposition; bone marrow biopsy is usually necessary. The biopsy demonstrates increased cellularity with a diffuse or occasionally patchy infiltrate with hairy cells. The infiltrate is loose and spongy, with pale-staining cytoplasm surrounding bland, monotonous round or ovoid nuclei.
Etiology No clear etiology Benzene exposure Radiation
The cytopenias are due to a combination of : *Bone marrow production failure caused by leukemic infiltration. *Hypersplenism. (increased destruction) Marrow failure may be due in part to*inhibitory factors (e.g., tumor necrosis factor) produced by the leukemic infiltrate,
Laboratory abnormalities in HCL is as follows: Anemia — 85% Thrombocytopenia — 80% Neutropenia — 80% Monocytopenia — 80% Azotemia — 30 % Abnormal liver function tests — 20% Hypergammaglobulinemia — 20% Leukocytosis (WBC >10,000) 10 to 20%
The mucosal lymphocyte antigen, CD103: is a sensitive marker for HCL. is a member of the integrin family The presence of CD103 , when coexpressed, is highly suggestive of HCL
In HCL: Vasculitis. Arthritis. Polyarthritis nodosa. Systemic Vasculitis. Many patients complaint: Arthitis or arthralgia.
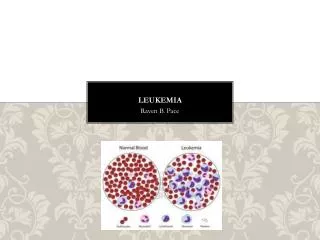
Diagnosis: Examination of the blood often suggests the diagnosis of HCL. In addition to the cytopenias the peripheral blood film usually demonstrates relative or absolute lymphocytosis, composed of cells with cytoplasmic projections, giving rise to the name hairy cell leukemia
patients often experience repeated infections and, more rarely, a systemic vasculitis Resembling polyarteritis nodosa
TRAP test Hairy cells exhibit a strong acid phosphatase (isoenzyme 5). Cytochemical reaction in more 95% of cases, a reaction that is resistant to the inhibitory effect of tartaric acid (TRAP).
Hairy cells expressCD19, CD20, CD22CD25 , CD11C , CD103 , FMC7, but not CD21 or CD5. Cell-surface immunoglobulins can be immunoglobulin G (IgG) or immunoglobulin A (IgA), The cells demonstrate a κ or λ light-chain phenotype
Clinical presentation *Abdominal fullness or discomfort dueto *Splenomegaly, which may be massive. *Systemic complaints (eg, fatigue, weakness, and weight loss). *Bruising and bleeding *Recurrent infections, which may be life- threatening, secondary to granulocytopenia and monocytopenia. *Splenomegaly or cytopenias
Annexin A1 : HCL has a gene expression profile that is distinct from that of other B cell lymphomas, including overexpression of the ANXA1 gene (annexin A1)
DIFFERENTIAL DIAGNOSIS 1-Small B cell lymphoproliferative disorders. associated with splenomegaly . 2-Chronic lymphocytic leukemia (CLL), 3-Prolymphocytic leukemia . The abnormal B cell in CLL usually stains positively for CD5, B cell CLL is usually negative for CD103, prolymphocytic leukemia present with splenomegaly, marked elevation of the white blood cell count, and the characteristic morphology of the prolymphocytes
Renal insufficiency in HCL due to: Infiltration Bleeding Infections Immune Complex Protein excertion Light chain deposition ( Nephrotic Syndrome) Acquired Fanconi’s syndrome ( Proximal renal tubules)
A Microbicidal defect of the neutrophils and aggregation defect of platelets have been reported in HCL
Patients with HCL have a predilection to develop tuberculosis , atypical mycobacterial infections, or fungal infections, perhaps related to the severe monocytopenia that is characteristic of this disorder. Pneumonia and septicemia are common causes of death in HCL.
(Treatment) Splenoctomy Interferon, 2-CDA, pentostatin Cladribine Granulocyte colony-stimulating factor (G-CSF) Rituximab Anti-CD20 antibody) Anti-CD22 antibody (BL22) Anti-CD25 antibody (LMB-2)
Splenectomy, often used in the past as the first treatment of most patients with complications from HCL, temporarily improves blood cell counts in two thirds of patients, usually within 1 to 4 weeks, but does not decrease the infiltration of hairy cells in the marrow or reduce the incidence of infections.
Treatment A small proportion (<5%) of patients with HCL do not require therapy. Splenectomy, often used in the past as the first treatment of most patients two thirds of patients, usually within 1 to 4 weeks, but does not decrease the infiltration of hairy cells in the marrow or reduce the incidence of infections. Splenectomy is recommended mainly for patients with splenic infarcts or massive splenomegaly.
2-Chlorodeoxyadenosine (2-CDA), an adenosine analogue deaminase , produces complete remissions in more than 90% of HCL patients with a single course of 0.1 mg/kg/day for 7 days by continuous intravenous infusion.
Effect of 2-CDA 2- CDA 0.1 mg/kg body weight per day by continuous intravenous infusion for seven days The complete and partial remission rates were 91%. The overall survival was 96% The relapse rates for patients achieving CR ( after 10Y) were 16 % .
Cladribine (2-CdA) Cladribine accumulates in lymphoid cells presumably because they are rich in deoxycytidine kinase. This enzyme phosphorylates cladribine, creating a deoxynucleotide that cannot readily exit the cell. The net effect is lymphotoxicity.
Cladribine and Pentostatin: In one study of 219 patients followed for a median period of 12.5 years, overall response rates (100 versus 96 percent), rates of complete remission 10-year survivals (100 versus 96 percent) were similar for initial treatment with either cladribine or pentostatin, respectively.
Side effects: Both Cladribine and Pentostatin produce prolonged immunosuppression Opportunistic infections, Herpes zoster
Treatment Relapsed HCL Retreatment with a second cycle of Cladribine or Pentostatine leads to a second complete remission in up to 70 percent of patients