Download

1 / 25

E N D
Legislation and the establishment of an open and learning culture in health careHenning Boje Andersen1 and Niels Hermann21Risø National Laboratory, Roskilde, Denmark2 National Board of Health, Copenhagen, DenmarkAnnual Conference of the Society for Risk Analysis - Europe:INNOVATION AND TECHNICAL PROGRESS: BENEFIT WITHOUT RISK?11-13 September 2006, Ljubljana, Slovenia
National project prior to legislation Nationally funded project 2001-02: • Focus group interviews with doctors and nurses • Questionnaire survey • Overview of international literature on reporting systems in medicine and other domains • Recommendations for a reporting system at the national level and local levels Prooject partners: DSI Institute of Health Care; Danish Inst. of Medical Simulation, Herlev Hospital; Risø National Lab., Denmark
Project background & impact Background: Rise in awareness in DK about patient safety in 2000/2001 Project received support from: The Danish Ministry of the Interior and Health and County of Copenhagen Impact: Project recommandation have been incorporated in the proposal for a new law in Denmark about adverse incident reporting and the support of learning systems
Survey: Data collection (1:2) Doctors and nurses employed in all hospitals in 4 Danish Counties,Jan.- Feb. 2002 Respondents recruited from • University Hospitals of Copenhagen County (about 1/3) • All General Hospitals in 3 counties (nearly 2/3) Major specialties included - distinguishable in data: • Anaesthesiology • Internal medicine • Orthopedic surgery • General surgery • Gynecology
The survey instrument: Adverse Events Questionnaire (AEQ) • Four cases UK case about disclosure to the pt; a near-miss incident a mild outcome incident; and a severe outcome event • Models of reporting • Reasons for not reporting • Patients’ requirements • Reactions (pos/neg) towards staff from leaders • Attitudes to errors and factors impacting on safety
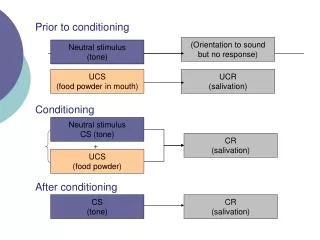
Three Models of Reporting • Anonymity: reporter not known to anyone else – written, unsigned report • Strict confidentiality:reporter known only to person(s) appointed as ”receiver” • Limited confidentiality:identity of reporter known only to ”receiver”, but revealed to authorities if event involves ”gross negligence” or a crime
Reasons for not reporting (1:2) • We have no tradition in my department for bringing up adverse events/errors • When I am busy I forget to bring up adverse events/errors • The patient may file a complaint • I don’t know who is responsible for bringing up adverse events/errors • I might get a reprimand • It might have consequences for my future employment or career • It wouldn’t help the patients that I bring up my own events/errors
Reasons for not reporting (2:2) • It might get out and the press might start writing about it • The adverse event/error may become reported to the medical licensing board • It is too cumbersome to bring up adverse events/errors • One does not feel confident about bringing up adverse events/errors in our department • I do not wish to appear as an incompetent doctor [nurse] • Bringing up adverse events/errors is not going to lead to any improvement in our ward/dept.
The project group’s recommendations: • strictlyconfidential reporting • name/identity not disclosed outside the ward / department • sharp distinction between disciplinary and learning functions of reporting • mandatory reporting of critical events • in addition, discretionary reporting to be encouraged • reporting made locally, enabling dialogue with and feedback to the reporting staff • data transmitted in an anomymous format into a national database of adverse events
Project results and Legislation • Main finding: A definite willingness to report adverse events into some type of confidential system • At the time of the survey, no system to receive event reports for learning and patient safety • Recommendations incorporated into Danish Patient Safety Act (January 2004): • personnel are required to report • personnel may not be subjected to investigation or disciplinary action on the basis of reporting • reporting is confidential or anonymous as chosen by reporting health care staff member
Does the legislation and its implementation live up to expectations?
Increasing number of reports received during the first two years of operation Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 2004 2005
Safety Assessment Codes (SAC scores)[Veterans Health Administation]
How does the new system perform? • Receives very large number of reports • Considerable activity at local and regional levels – though varying across counties • National intiatives especially via the Danish Patient Safety Society • Feedback and alerts primarily from local/regional level • Next step: extension to health sector outside hospitals