Download
1 / 19
190 likes | 364 Views
An Overview of Anterior Cruciate Ligament Injuries. PAS 646 March 30, 2006 Advisor: Samuel Powdrill, M.Phil, PA-C Kurt Kramer. Background. Anatomy of the knee Epidemiology Mechanism of injury Risk factors Presentation of injury Diagnosis Rehabilitation (“prehab” vs. “rehab”)

E N D
An Overview of Anterior Cruciate Ligament Injuries PAS 646 March 30, 2006 Advisor: Samuel Powdrill, M.Phil, PA-C Kurt Kramer
Background • Anatomy of the knee • Epidemiology • Mechanism of injury • Risk factors • Presentation of injury • Diagnosis • Rehabilitation (“prehab” vs. “rehab”) • Graft choices • Surgical technique • Prevention
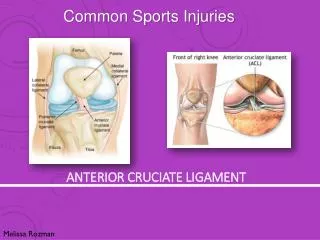
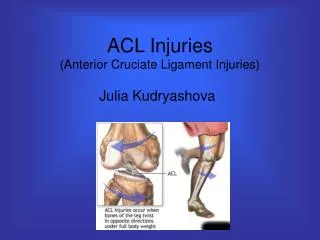
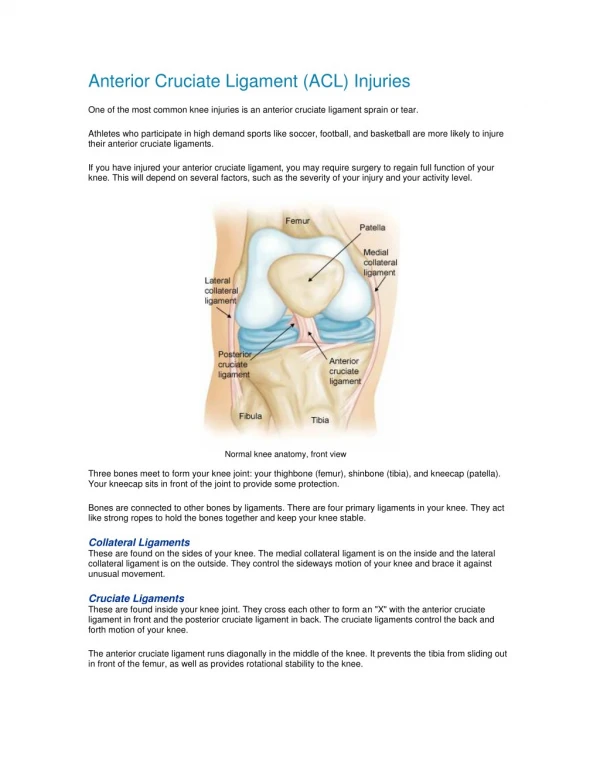
Discussion • Knee Anatomy • Anterior cruciate ligament (ACL) one of four stabilizing ligaments • Protects integrity of menisci and articular cartilage • ACL prevents excessive anterior translation of the tibia and internal or external rotation of the tibia on the femur
Discussion cont’d • Anatomy • Normal ACL viewed arthroscopically
Discussion cont’d • Epidemiology • Annual incidence of ~200,000 ACL ruptures per year with an estimated 1 in 3,000 • Females > Males • Incidence highest in population aged 15-45 years old with 1 in 1750 persons (Brown, 2004) • Repair is now being indicated in older populations to prevent earlier onset of osteoarthritis • Average return to full activity is ~ 6 to 8 months
Discussion cont’d • Mechanism of Injury • Usually a hx of non-contact injury (70%) • Common is any physical activity that requires quick change in direction or a contact sport • Soccer, basketball, volleyball, football, and skiing • Mechanism usually involves sudden deceleration, hyperextension, and tibial torsion
Discussion cont’d • Risk Factors • Individuals participating in high risk sports • Playing surface • High shoe-surface friction that increase performance (artificial turf) • Neuromuscular deficits of the female sex • Increased incidence of female injury is NOT associated with sex specific hormones • Females tend to activate their quadriceps near full knee extension, thus landing with smaller angles of knee flexion than their male counterpart • Females show earlier neuromuscular fatigue
Discussion cont’d • ACL Injury Presentation • History is key! • Know the mechanism of ACL injuries! • Appropriate mechanism accompanied by what patient describes as a “pop” and excruciating pain • Excessive swelling with knee effusion • Decreased range of motion (ROM) • Inability to contract quadriceps • H-reflex
Discussion cont’d • Diagnosis • History and presentation • + Lachman’s or Anterior Drawer • Imaging • X-ray (avulsion) • MRI • Hemarthrosis (joint aspiration) • Appropriate referral
Discussion cont’d • Rehabilitation • Prehab (Gold-standard) • Implemented immediately after diagnosis • Decrease pain and swelling • Increase ROM, quad strength, and proprioception >90% of contralateral leg • Prehab allows for quicker post-operative return to ADLs and physical activity • Rehab • Progression varies depending on graft choice • Also focuses on decreasing pain and swelling, while increasing ROM, strength, and proprioception
Discussion cont’d • Graft choices (4 most commonly used) • Achilles tendon allograft • Used in pts. whom desire less painful recovery, improved cosmetic appearance, lead a less active lifestyle, and those with no other available graft choice • Cole et al. 2005 report that pts. had significantly less pain when compared to bone-patellar tendon-bone (BPTB) autograft (P<.0001) • Increased risk of infection, immunologic response, and alteration of graft structural properties by sterilization, thus affecting long-term graft stability has deterred most surgeons from choosing this graft (Shelbourne 2002; Beynnon et al. 2005)
Discussion cont’d • Hamstring tendon autograft • Harvested from the semitendonosis or gracilis tendon from the ipsilateral leg • Some physicians prefer this graft due to pts. reporting patellofemoral pain with the BPTB autograft (Goldblatt 2005), while Svenson et al. report no significant difference in levels of pain b/w this graft and the BPTB autograft • Svenson et al. report increased laxity with hamstring autograft when compared to pts. that received a BPTB autograft • Freedman et al. report significantly lower graft failure (P<.001), significantly better static knee stability (P<.017), and higher patient satisfaction (P<.001) with the use of BPTB autograft when compared to hamstring autografts
Discussion cont’d • Ipsilateral BPTB autograft • Preferred graft of choice among surgeons (Shelbourne 2000) • Offers greater static stability than non-BPTB grafts due to bone-to-bone contact in the metaphyseal region of the tibia and femur (Shelbourne 1999; Yunes et al. 2001) • Increased graft stability post-op when compared to hamstring autograft (Shelbourne 2000) • Roe et al. reports increased ant. knee pn with BPTB autograft and increased prevelance of osteoarthritis at 7 yrs. post-op
Discussion cont’d • Contralateral BPTB autograft • Many of same benefits and disadvantages as ipsilateral BPTB autograft • If combined with appropriate accelerated rehabilitation program may allow athlete to return to full activity 4 wks. post-op without an increased risk loss of stability or early graft tear (Shelbourne 2002) • Theory of contralateral BPTB autograft is that by dividing the trauma of surgery and rehab b/w both extremities, evidence shows course of rehab is easier, quicker, and more reliable (Shelbourne 2002) • Slightly longer operating time, increased patient education, and new approach to rehab for athletic trainers and PTs • Safe and predictable return without sacrificing strength, ROM, and stability • Used in patients in which return to sports is a priority
Discussion cont’d • Surgical Technique • Harvest graft • Expose joint • Remove damaged ACL, clean, and make room for new ACL • Drill tibial and femoral tunnels • Insert new ACL with bone plugs (button approach shown)
Discussion cont’d • Prevention • ACL injury prevention programs • Programs focus on modifying neuromuscular and biomechanical risk factors • Agility drills and plyometric exercises • Recognition of injury associated actions and positions • Educate athletes in proper jumping techniques, softer landings, instant recoil, and correct posture and alignment • Significantly decreased incidence of ACL injuries among female high school soccer, basketball, and volleyball athletes (Brown 2004); thus supporting the theory that there are neuromuscular risk factors associated with the frequency of ACL tears
Conclusion • Important for PCP to have thorough understanding of anatomy, mx of injury, special testing, and appropriate tx or referral • Appropriate referral may be key to full return to activity and long-term patient satisfaction (everyone is different) • Be familiar with orthopedic surgeons in area and what protocols and grafting options they utilized • Pts. lead different lifestyles, thus one protocol and graft choice will likely be more appropriate treatment for one pt. than another • More research needed for long-term graft stability and pt. satisfaction for each graft • Swallow your pride and utilize local PTs and ATCs!
References • Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Treatment of anterior cruciate ligament injuries, Part 1. Am J Sports Med 2005; 33: 1579-1602. • Brown JR, Trojian TH. Anterior and posterior cruciate ligament injuries. Prim Care Clin Office Pract 2004; 31: 925-56. • Cole DW, et al. Cost comparison of anterior cruciate ligament reconstruction: autograft versus allograft. Arthroscopy 2005; 21: 786-90. • DeCarlo M, Shelbourne KD, Oneacre K. Rehabilitation program for both knees when the contralateral autogenous patellar tendon graft is used for primary anterior cruciate ligament reconstruction: a case study. J Orthop Sports Phys Ther 1999; 29: 144-53. • Freedman KB, D’Amato MJ, Nedeff DD, et al. Arthroscopic Anterior Cruciate Ligament Reconstruction: A meta-analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med 2003; 31: 2-11. • Goldblatt JP, Fitzsimmons SE, Balk E, et al. Reconstruction of the anterior cruciate ligament: meta-analysis of patellar tendon versus hamstring tendon autograft. Arthroscopy 2005; 21: 791-803. • Jari S, Shelbourne KD. Simultaneous bilateral anterior cruciate ligament reconstruction. Am J Sports Med 2002; 30: 891-4. • Johnson DH, Maffulli N, King JB, et al. Anterior cruciate ligament reconstruction: A cynical view from the British Isles on the indications of surgery. Arthroscopy 2003; 19: 203-9. • Malinzak RA. Mechanisms of ACL injuries. Coach Kryzewski Human Performance Laboratory. K-Lab Symposium in Sports Performance Enhancement Workshop, Duke University Medical Center, Department of Sports Medicine-Orthopaedic Surgery, July 10th, 1999. • Mastrokalos DS, Springer J, Siebold R, et al. Donor site morbidity and return to the preinjury activity level after anterior cruciate ligament reconstruction using ipsilateral and contralateral patellar tendon autograft: a retrospective, nonrandomized study. Am J Sports Med 2005; 33: 85-93. • Poehling GG, Curl WW, Lee CA, et al. Analysis of outcomes of anterior cruciate ligament repair with 5-year follow-up: allograft versus autograft. • Roe J, Pinczewski LA, Russell VJ, et al. A 7-year follow-up of patellar tendon and hamstring tendon grafts for arthroscopic anterior cruciate ligament reconstruction. Am J Sports Med 2005; 33: 1337-45. • Shelbourne KD, Rask BP. Controversies with anterior cruciate ligament surgery and rehabilitation. Am J of Knee Surgery 1998; 11: 136-43. • Shelbourne KD, Johnson BC. Effects of patellar tendon width and preoperative quadriceps strength on strength after anterior cruciate ligament reconstruction with ipsilateral bone-patellar tendon-bone autograft. Am J Sports Med 2004; 32: 1474-8. • Shelbourne KD, Davis TJ. Evaluation of knee stability before and after participation in a functional sports agility program during rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1999; 27: 156-61. • Shelbourne KD, Beaty JH. Graft selection for ACL reconstruction: Contralateral patellar tendon autograft (Instructional Course Lectures). Am Academy of Ortho Surg 2002; 51: 325-328. • Shelbourne KD, Urch SE. Primary anterior cruciate ligament reconstruction using the contralateral autogenous patellar tendon. Am J Sports Med 2000; 28: 651-8. • Wilk KE, Reinold MM, Hooks TR. Recent advances in the rehabilitation of isolated and combined anterior cruciate ligament injuries. Orthop Clin N Am 2003; 34: 107-37. • Yunes M, Richmond JC, Engels EA, et al. Patellar versus hamstring tendons in anterior cruciate ligament reconstruction: A meta-analysis. • Zink EJ, Trumper RV, Smidt CR, et al. Gender comparison of knee strength recovery following ACL reconstruction with contralateral patellar tendon. Biomed Sci Instrum 2005; 41: 323-8.