Download
1 / 1
10 likes | 118 Views
Abstract. Results. Study Design. Discussion.

E N D
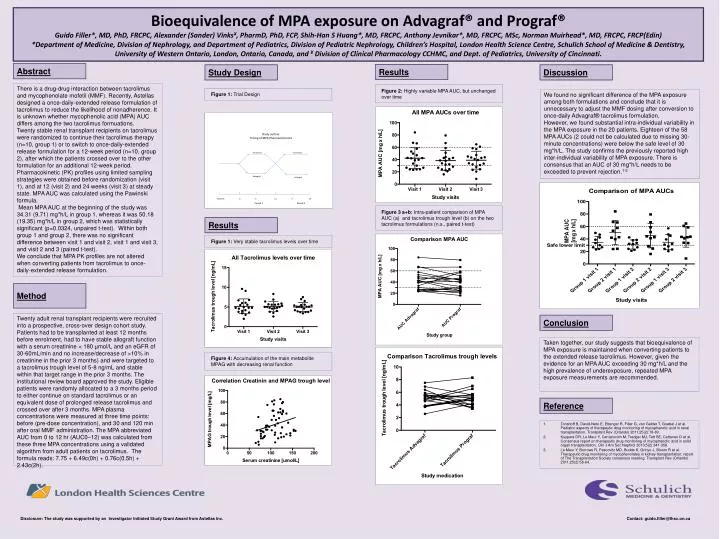
Abstract Results Study Design Discussion There is a drug-drug interaction between tacrolimus and mycophenolate mofetil (MMF). Recently, Astellas designed a once-daily-extended release formulation of tacrolimus to reduce the likelihood of nonadherence. It is unknown whether mycophenolic acid (MPA) AUC differs among the two tacrolimus formuations. Twenty stable renal transplant recipients on tacrolimus were randomized to continue their tacrolimus therapy (n=10, group 1) or to switch to once-daily-extended release formulation for a 12-week period (n=10, group 2), after which the patients crossed over to the other formulation for an additional 12-week period. Pharmacokinetic (PK) profiles using limited sampling strategies were obtained before randomization (visit 1), and at 12 (visit 2) and 24 weeks (visit 3) at steady state. MPA AUC was calculated using the Pawinski formula. Mean MPA AUC at the beginning of the study was 34.31 (9.71) mg*h/L in group 1, whereas it was 50.18 (19.35) mg*h/L in group 2, which was statistically significant (p=0.0324, unpaired t-test). Within both group 1 and group 2, there was no significant difference between visit 1 and visit 2, visit 1 and visit 3, and visit 2 and 3 (paired t-test). We conclude that MPA PK profiles are not altered when converting patients from tacrolimus to once-daily-extended release formulation. Figure 2: Highly variable MPA AUC, but unchanged over time Figure 1: Trial Design We found no significant difference of the MPA exposure among both formulations and conclude that it is unnecessary to adjust the MMF dosing after conversion to once-daily Advagraf® tacrolimus formulation. However, we found substantial intra-individual variability in the MPA exposure in the 20 patients. Eighteen of the 58 MPA AUCs (2 could not be calculated due to missing 30-minute concentrations) were below the safe level of 30 mg*h/L. The study confirms the previously reported high inter-individual variability of MPA exposure. There is consensus that an AUC of 30 mg*h/L needs to be exceeded to prevent rejection.1-3 Bioequivalence of MPA exposure on Advagraf® and Prograf® Guido Filler*, MD, PhD, FRCPC, Alexander (Sander) Vinks¥, PharmD, PhD, FCP, Shih-Han S Huang*, MD, FRCPC, Anthony Jevnikar*, MD, FRCPC, MSc, Norman Muirhead*, MD, FRCPC, FRCP(Edin) *Department of Medicine, Division of Nephrology, and Department of Pediatrics, Division of Pediatric Nephrology, Children’s Hospital, London Health Science Centre, Schulich School of Medicine & Dentistry, University of Western Ontario, London, Ontario, Canada, and ¥ Division of Clinical Pharmacology CCHMC, and Dept. of Pediatrics, University of Cincinnati. Figure 3 a+b: Intra-patient comparison of MPA AUC (a) and tacrolimus trough level (b) on the two tacrolimus formulations (n.s., paired t-test) Results Figure 1: Very stable tacrolimus levels over time Method Twenty adult renal transplant recipients were recruited into a prospective, cross-over design cohort study. Patients had to be transplanted at least 12 months before enrolment, had to have stable allograft function with a serum creatinine < 180 µmol/L and an eGFR of 30-60mL/min and no increase/decrease of >10% in creatinine in the prior 3 months) and were targeted to a tacrolimus trough level of 5-8 ng/mL and stable within that target range in the prior 3 months. The institutional review board approved the study. Eligible patients were randomly allocated to a 3 months period to either continue on standard tacrolimus or an equivalent dose of prolonged release tacrolimus and crossed over after 3 months. MPA plasma concentrations were measured at three time points: before (pre-dose concentration), and 30 and 120 min after oral MMF administration. The MPA abbreviated AUC from 0 to 12 hr (AUC0–12) was calculated from these three MPA concentrations using a validated algorithm from adult patients on tacrolimus. The formula reads: 7.75 + 6.49c(0h) + 0.76c(0.5h) + 2.43c(2h). Conclusion Taken together, our study suggests that bioequivalence of MPA exposure is maintained when converting patients to the extended release tacrolimus. However, given the evidence for an MPA AUC exceeding 30 mg*h/L and the high prevalence of underexposure, repeated MPA exposure measurements are recommended. Figure 4: Accumulation of the main metabolite MPAG with decreasing renal function Reference 1. Tonshoff B, David-Neto E, Ettenger R, Filler G, van Gelder T, Goebel J et al. Pediatric aspects of therapeutic drug monitoring of mycophenolic acid in renal transplantation. Transplant Rev (Orlando) 2011;25(2):78-89. 2. Kuypers DR, Le Meur Y, Cantarovich M, Tredger MJ, Tett SE, Cattaneo D et al. Consensus report on therapeutic drug monitoring of mycophenolic acid in solid organ transplantation. Clin J Am SocNephrol 2010;5(2):341-358. 3. Le Meur Y, Borrows R, Pescovitz MD, Budde K, Grinyo J, Bloom R et al. Therapeutic drug monitoring of mycophenolates in kidney transplantation: report of The Transplantation Society consensus meeting. Transplant Rev (Orlando) 2011;25(2):58-64. Disclosure: The study was supported by an Investigator Initiated Study Grant Award from AstellasInc. Contact: guido.filler@lhsc.on.ca