Download
1 / 3
70 likes | 376 Views
Accordion Grading System. Mild Complications Requires only minor invasive procedures that can be done at the bedside such as insertion of intravenous lines, urinary catheters, and nasogastric tubes, drainage of wound infections and antiemetics, antipyretics, analgesics and electrolytes.

E N D
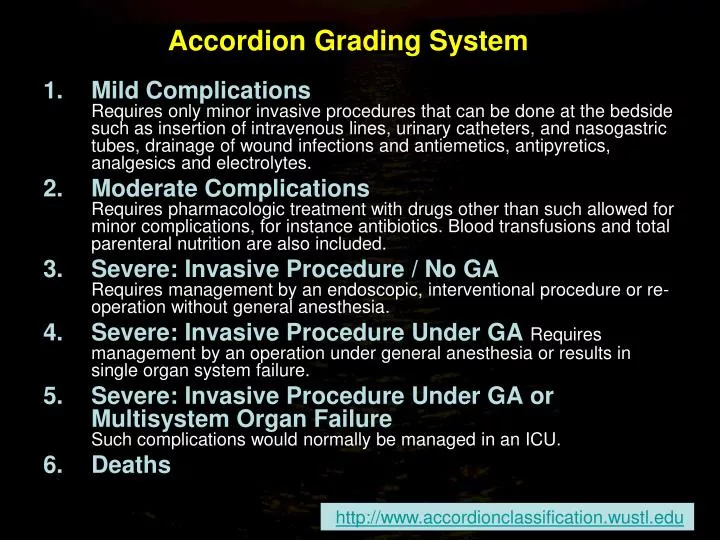
Accordion Grading System Mild ComplicationsRequires only minor invasive procedures that can be done at the bedside such as insertion of intravenous lines, urinary catheters, and nasogastric tubes, drainage of wound infections and antiemetics, antipyretics, analgesics and electrolytes. Moderate ComplicationsRequires pharmacologic treatment with drugs other than such allowed for minor complications, for instance antibiotics. Blood transfusions and total parenteral nutrition are also included. Severe: Invasive Procedure / No GARequires management by an endoscopic, interventional procedure or re-operation without general anesthesia. Severe: Invasive Procedure Under GA Requires management by an operation under general anesthesia or results in single organ system failure. Severe: Invasive Procedure Under GA or Multisystem Organ FailureSuch complications would normally be managed in an ICU. Deaths http://www.accordionclassification.wustl.edu
Accordion Severity Classification of Postoperative Complications (ASCPC): Contracted Classification Grado 1: Complicanza lieveRichiede soltanto procedure invasive minori che possono essere fatte a letto del paziente come inserzione di vie endovenose, cateteri urinari, sondini naso-gastrici e drenaggio di ferite. Sono ammessi farmaci antiemetici, antipiretici, diuretici, analgesici, elettroliti e la fisioterapia Grado 2: Complicanza mediaRichiede trattamenti farmacologici diversi da quelli richiesti dalle complicanze minori come antibiotici, trasfusioni e NPT Grado 3: Complicanza severaTutte le complicanze che richiedono trattamenti endoscopici, procedure di radiologia interventistica o reinterventi o complicanze che causano deficit di uno o più organi, ricovero in ICU Grado 4: MorteDecesso postoperatorio Strasberg SM et al. Ann Surg 250(2): 177-186, 2009
DeOliveira e coll. Annals of Surgery 244: 931-939, 2006 Una larga implementazione del grading permetterebbe una valutazione obiettiva ed omogenea dei risultati. La qualifica di “centro di eccellenza” dovrebbe riflettere l’obiettiva valutazione delle complicanze e della mortalità