Download
1 / 69
760 likes | 1.06k Views
Executive Dysfunction and Language Impairment in Frontotemporal Dementia. Sandra Hogsed, MS, CCC-SLP Western Carolina University November 9, 2010. What is Frontotemporal Dementia?.

E N D
Executive Dysfunction andLanguage Impairment in Frontotemporal Dementia Sandra Hogsed, MS, CCC-SLP Western Carolina University November 9, 2010
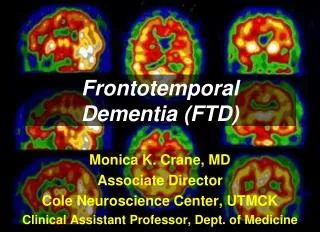
What is Frontotemporal Dementia? “Frontotemporal dementia (FTD), or referred to as frontotemporal lobar degeneration (FTD), is a group of related conditions resulting from the progressive degeneration of the temporal and frontal lobes of the brain. These areas of the brain play a significant role in decision-making, behavioral control, emotion and language.” Frontotemporal Dementia, University of California, San Francisco, Memory and Aging Center, http://memory.ucsf.edu/ftd/.
Disease Onset • FTD usually first appears when someone is in their mid-40s to early-60s and causes a steady, gradual decline in the ability to complete the daily activities of life. The disease can last anywhere from three to 17 years from the first symptom until death, with an average duration of eight years after diagnosis. FTD occurs equally in men and women. In a small percentage of cases it is inherited. • The Association for Frontotemporal Dementias, • http://www.ftd-picks.org/
Prevalence • FTD represents an estimated 10%-20% of all dementia cases and is recognized as one of the most common dementias affecting a younger population. It is estimated that FTD affects approximately 250,000 Americans. The Association for Frontotemporal Dementias, http://www.ftd-picks.org/
Normal Brain vs. FTD Image retrieved on 9/19/10 from http://www.riversideonline.com
Types of FTD The term "frontotemporal dementia" (FTD) includes several different clinical subtypes: • Behavioral variant FTD- "frontal variant FTD" or "pick's disease" • Semantic dementia- “temporal variant FTD” • Progressive non-fluent aphasia • FTD with motor neuron disease, which includes corticobasal degeneration, progressive supranuclear palsy and motor neuron disease. The specific areas of the brain affected by each subtype cause different symptoms. Frontotemporal Dementia, University of California, San Francisco, Memory and Aging Center, http://memory.ucsf.edu/ftd/.
Behavioral Variant FTDSymptoms • Behavioral and personality changes • Decreased concern for social norms • Disinhibition and loss of personal control • Lack of insight into their own behaviors, denial of deficits • Lack of responsibilities • Withdrawal and apathy • Increased appetite for sweets • Personal hygiene deterioration • Hypersexual behavior • Compulsiveness, perseverations or stereotyped repetitive acts Bozeat, S., Gregory, C., Lambon, R., & Hodges, J. (2000). Which neuropsychiatric features distinguish frontal and temporal variants of frontotemporal dementia from Alzheimer’s disease? Journal of Neurology, Neurosurgery, and Psychiatry, 69, 178-186. Hodges, J. & Miller, B. (2001). Classification, genetics and neuropathology of frontotemporal dementia. Introduction to the special topics papers, part 1 (Review) Neurocase, 7, 31-35. Neary, D., Snowden, J., Gustafson, L., Passant, U., Stuss, D., Black, S., Freedman, M., et al. (1998). Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology, 51, 1546-1554.
Semantic Dementia • Word-finding difficulties • Fluent aphasia • Anomia • Impaired comprehension of word meaning • Inability to match semantically-related pictures or objects As the disease progresses, behavioral and personality changes similar to the behavioral variant FTD may become apparent. The Association for Frontotemporal Dementias, http://www.ftd-picks.org/
Progressive Non-Fluent Aphasia • Hesitant, effortful speech • Relatively preserved comprehension of speech • Relatively preserved reading and writing abilities • Increased difficulty with production of speech related to weakness and incoordination • Speech that sounds imprecise and uncoordinated • Difficulty with swallowing The Association for Frontotemporal Dementias, http://www.ftd-picks.org/
Motor Neuron Disease • Muscle weakness, which can involve the arms, legs, face, tongue or neck • Clumsiness, or difficulty with fine motor movements of the hands • Tripping or falling due to weak or stiff legs • Shortness of breath due to weak muscles in the diaphragm • Muscle atrophy • Fasciculations • Muscle cramps • Dysphagia • Dysarthria • Spasticity • Hyperreflexia- exaggerated reflexes • Uncontrollable outbursts of laughing or crying The Association for Frontotemporal Dementias, http://www.ftd-picks.org/
To summarize…what cognitive domains are affected by FTD? • Receptive Language • Memory and Learning • Thinking • Expressive Language • Attention • Executive Functioning and Reasoning
Videos about FTD Caregivers of FTD • http://www.youtube.com/watch?v=dP4PoUkVy0U Frontotemporal Dementia (Mayo Clinic) • http://youtu.be/EHSdNjhkvE8 • Does the young person with behavior variant FTD remind you of another disorder?
Pathology of FTD Pathology occurs with degeneration and gliosis. This begins in the orbitofrontal cortex of the brain. • Degeneration results in abnormally folded protein “clumps.” One type of inclusion is called the Pick body, named for the neurologist who first described this disease, Arnold Pick. • Gliosis develops in the damaged region. The posterior part of the brain is spared in FTD, so many day-to-day functions are normal in the early stages. Rosen, H., Hartikanen, K., Jaqust, W., Kramer, J., Reed, B., Cummings, J., Boone, K., Ellis, W., Miller, C., Miller, B. (2002). Utility of clinical criteria in differentiating frontotemporal lobar degeneration (FTD) from AD. Neurology, 58, 1585-1586.
Tauopathy At least two different disease proteins are implicated in FTD pathology. These include tau and TDP-43. FTD-Tau FTD -TDP The protein tau is found to be responsible in the disease process, such as when it accumulates as aggregates in Pick’s disease, corticobasal degeneration and progressive supranuclear palsy. A proteinopathy that results when abnormal TDP-43 protein accumulates in nerve cells. Yoshiyama, Y., Lee, V., Trojanowski, J. (2001) Frontotemporal dementia and tauopathy. Current Neurology and Neuroscience Reports, 1, 413-421.
Genetics • A subset of patients with FTD-TAU and FTD-TDP have a family history and genetic mutations have been identified. These inherited cases of FTD-TAU are associated with mutations in the tau gene where as FTD-TDP cases may be associated with abnormalities of the progranulin gene or the TDP-43 gene. Geser, F., Martinez-Lage, M., Kwong, L., Lee, V., Trojanowski, J. (2009) Amyotrophic lateral sclerosis, frontotemporal dementia and beyond: the TDP-43 diseases. Journal of Neurology, 256:1205–1214. Murray, B., Lynch, T., Farrell, M. (2005) Clinicopathological features of the tauopathies. Biochemical Society Transaction, 33, 4.
Tauopathy Image retrieved on 9/19/2010 from http://ellisonfoundation.org
Brain Location and Symptoms Behavioral (Frontal) Aphasic (Temporal) Orbitofrontal lobe dysfunction- early personality change and disinhibition Medial frontal (anterior cingulate)-apathy, abulia, mutism, apraxia, perseveration Dorsolateral frontal lobe- disorganization and sequential organization Non-dominant anterior temporal lobe-selfishness/callousness, antisocial traits, lack of empathy, new artistic or musical talent Dominant posterior temporal or inferior frontal lobe- halting, agrammatic speech with frequent paraphasic errors but relatively preserved comprehension Temporal- semantic dementia- impaired comprehension and word-finding deficits Murray et al., (2005)
FTD Progression “As FTD progresses, the various subtypes merge so that patients develop combinations of clinical syndromes and eventually progress to a global dementia.” Murray, et al., (2005)
Subtypes of FTD eventually merge Murray, et al. (2005) Image retrieved on 11/05/10 from http://www.biochemsoctrans.org
Journal Article #1 Torralva, T., Roca, M., Gleichgerrcht, E. , Bekinschtein, T., and Manes, F. (2009) A neuropsychological battery to detect specific executive and social cognitive impairments in early frontotemporal dementia, Brain, 132; 1299-1309.
Question? • Traditional cognitive tests may not be sensitive to the early identification of bvFTD. This study aimed to identify specific neuropsychological tests that were particularly sensitive to identification of the specific executive and social cognitive deficits in those with early bvFTD. Torralva, et al. (2009)
Classical Cognitive Measures • Wisconsin Card Sorting Test • Verbal fluency tests, or the Trail Making Test These may fail to detect the dysexecutive syndrome shown by these early bvFTD patients in everyday life (Gregory et al., 1999, 2002).
New Criteria for Diagnosis • There has been a recent revision of diagnostic and research criteria for bvFTD. Deficits in executive and social cognition tasks are now considered a core feature in its entirety. • The presence and detection of executive and social dysfunction may be particularly useful for diagnosis during the early stages of the disease. Kipps and Hodges (2006) Rascovsky, et al. (2007). Hodges, (2007)
Although severe deficits in various aspects of social cognition (i.e. Theory of Mind) and complex decision-making tend to appear in early stages of bvFTD, these domains are not often part of the assessment. Gregory et al., (2002); Torralva et al., (2007).
Purpose • This study attempted to enhance the traditional cognitive assessment battery with the addition of more comprehensive tests of complex executive social functioning to increase sensitivity for the detection of executive and social cognitive impairment in patients with early bvFTD.
New Proposed BatteryTests that measure performance of “daily life” activities within a “real life” environment; combined with traditional cognitive tests to increase sensitivity for the detection of executive and social cognitive impairment in patients with early bvFTD. • Multiple Errands Test (Burgess, 2002) • Hotel Task (Manly et al., 2002) • complex decision making (Iowa Gambling Task) (Bechara et al., 1994) • social cognition (Theory of Mind tests) (Baron-Cohen, 1997; Stone et al., 1998).
Methods • 35 bvFTD patients with early/mild stages of the disease, fulfilled Lund and Manchester criteria for bvFTD diagnosis (Neary et al., 1998). • Dementia severity was assessed using the Clinical Dementia Severity Rating Scale (CDR) (Hughes et al., 1982). • All patients underwent a standard examination battery including neurological, neuropsychiatric and neuropsychological examinations and a MRI-SPECT. • All patients showed frontal atrophy on MRI, and frontal hypoperfusion on SPECT, when available. • Only patients with frontal lobe atrophy were included in this study although the current diagnostic criteria does not specify need.
General Neuropsychological Battery • Addenbrooke’s Cognitive Examination (ACE) and the Mini Mental State Exam (MMSE; Folstein et al., 1975). • Premorbid IQ - Buenos Aires Word Accentuation Test (WAT-BA; Burin et al., 2000). • Attention and concentration- forward digit span task (Wechsler, 1991) and the Trail Making Test Part A (TMT-A; Partington and Leiter, 1949). • Memory- logical memory subtest from the Wechsler Memory Scale-Revised (Wechsler, 1991). • Language comprehension- adapted version of the Token Test (Spreen and Benton, 1977). • Naming assessed with the adapted version of the Boston Naming Test (Kaplan et al., 1983).
Proposed Executive and Social Cognition Battery (ESCB) • The Frontal Assessment Battery test (FAB; Dubois et al., 2000). • Backward digit span (Wechsler, 1991) • Letters and Numbers (Wechsler, 1939) • Word Fluency Tests • Trail Making Tests Part B (Partington, 1949) • Modified Wisconsin Card Sorting Test (Nelson, 1976) • Executive and social cognition battery (ESCB) • Multiple Errands Test Hospital Version (Shallice and Burgess, 1991) • The Hotel Task (Manly et al., 2002) • Iowa Gambling task (Bechara et al., 1994) • The Mind in the Eyes Test (Baron-Cohen et al., 1997) • Faux Pas Test (Stone et al., 1998).
Results • 16 participants with scores above 86 (hiACE) • 19 participants with a score of 86 or below (loACE). • By classifying bvFTD as being either above (hiACE) or below (loACE) the cut-off score of the Addenbrooke’s Cognitive Examination (ACE), the researchers were able to show that the hiACE group performed significantly below the healthy controls on the tests of the battery proposed, but did not differ on most of the standard (or classical) tests • Performance on every classical executive test included in the battery was significantly different for loACE compared to the control (CTR)
Statistical Analysis Participants clustered into 3 groups for statistical analysis • Healthy controls • bvFTD with an ACE score higher than 86 points • bvFTD with an ACE score of 86 points or less The score of 86 points (out of 100) was used, because it is accepted as the cut-off value of the ACE in diagnosing dementia (Mathuranath, et al., 2000).
Summary • Testing incorporated tasks that would resemble real-life demands, decision-making processes or social situations. • As expected the loACE group differed from healthy control on all measures of the ESCB. The hiACE group differed from controls in measures of real-life planning and organization, complex decision-making and theory of mind tests. This group made more errors than healthy controls (inefficiencies), acted more impulsively (rule breaks), with no apparent planning, and poor organization of the tasks (task failures).
“This study demonstrated that traditional measures of frontal executive function may be ineffective in the early detection of subtle executive and social cognition deficits in bvFTD. Patients with an apparent high performance on a standard neuropsychological test do not differ significantly from controls in their performance on basic cognitive domains or classical tests of executive function.” Torralva, et al. (2009)
Limitations • Diagnosis of bvFTD was based on clinical assessment alone and not on pathological analysis. • This study only tested specificity of global score in discriminating bvFTD from normal controls.
Journal Article #2 • Pakhamov, S., Smith, G., Chacon, D., Feliciano, Y., Radford, N., Caselli, R., Knopman, D. (2010) Computerized analysis of speech and language to identify psycholinguistic correlates of frontotemporal lobar degeneration, Cognitive and Behavioral Neurology, 23, 3, 165-177.
Question? • The purpose of this research was to evaluate the use of a semiautomated computerized system for measuring speech and language characteristics in patients with frontotemporal degeneration (FTD).
The need for improved definition of syndromes and phenotypes is a key theme in dementia research in general, and frontotemporal lobar degeneration (FTD) in particular.Currently, FTD comprises 3 syndromes: • Behavioral variant (bvFTD) • Progressive nonfluent aphasia • Semantic dementia The inclusion of progressive logopenic aphasia (PLA) as either a variant of FTD or Alzheimer is currently being debated.
Objective • Careful clinical evaluation is critical to FTD diagnosis, particularly in the early stages of disease progression. • A systematic analysis of spontaneous speech samples is considered “the single most valuable aspect of the diagnosis” for the aphasic FTD syndromes (Rohrer, et al.,2008). • Research in aphasia has contributed a set of instruments in the form of picture description tasks designed to elicit and rate spontaneous speech, including the Boston Diagnostic Aphasia Examination Cookie Theft stimulus.
Drawback of Traditional Measures? • Traditionally carried out manually. • The problem with this is the results are subjective and may not have the detail and precision to pick up on subtle nuances. • Detailed measurements of syntax, semantics, and prosody—the 3 areas identified in a survey of clinicians’ views on the clinical usefulness of aphasia test batteries. Beele, et. al, (1984).
Objective and Precise Instruments • Advances in computerized natural language processing (NLP) and automatic speech recognition (ASR) are making it possible to develop objective and precise instruments for automated or semiautomated analysis of speech and language. Hosom, J. Shriberg, L., & Green, J. (2004). Diagnostic assessment of childhood apraxia of speech using automatic speech recognition (ASR) methods. Journal of Medical Speech Language Pathology, 12, 167-171. Roark, B., Hosom, J., Mitchell, M., & Kaye, J. (2007). Automatically derived spoken language markers for detecting Mild Cognitive Impairment. Paper presented at the International Conference on Technology and Aging (ICTA).
Speech and Language Characteristics in Frontotemporal Lobar Degeneration • Progressive nonfluent aphasia- dysfluent, effortful, agrammatical speech. • Semantic dementia- nonverbal and verbal naming and recognition deficits with relatively preserved grammar. Despite these differences, there is considerable overlap between their language specific manifestations.
Language related deficits of bvFTD • In bvFTD, the language related deficits tend to be observed at the higher discourse level, rather than syntax, phonology, and semantics found with the other FTD variants. • Patients with bvFTD show impaired working memory that manifests itself through deficits in sentence comprehension (Cooke, et al., 2003), thematic role processing in verbs (Peele, et al.,2007; Murray, et al., 2007), and altered discourse characteristics (Ash, et al., 2006): discourse coherence, cohesion, and “empty” speech (overuse of pronouns) (Almor, et al.,2001; Almor, et al., 2001; Glosser, et al., 1991).
Problems in Current Diagnostic Techniques • Thompson et al (1997) suggested that neuropsychologic tests may be too narrow to capture the richness of the behavioral and cognitive features of FTD and even obscure the differences between patient groups.
Proposal • Qualitative assessments of error types were proposed to complement neuropsycologic test scores in obtaining a more complete characterization of FTD variants. This research was designed in hopes that computerized linguistics and NLP technology may help to quantify some of these qualitative measures.
Methods • 38 patients diagnosed with 1 of 3 FTD syndromes and PLA were recruited from 3 academic medical centers. • All 38 participants underwent neuropsychologic testing that included the Boston Diagnostic Aphasia Examination Cookie Theft Picture Description Task.
Diagnostic Criteria • Only patients with behavioral variant frontotemporal dementia (bvFTD), progressive non-fluent aphasia (PNFA), progressive logopenic aphasia (PLA), and semantic dementia (SD) were included in the study –based on Neary criteria (Neary et al., 1998). • All patients were required to have imaging studies showing focal cerebral atrophy of at least 1 of these: the anterior temporal lobes, frontal lobes, insula, or caudate nuclei.
Criteria for diagnosis of the FTD disorders • PNFA- diagnosed by expressive deficits of at least 3 of these: nonfluency, speech hesitancy or labored speech, word finding difficulty. • PLA- diagnosed with fluent aphasia with anomia but intact word meaning and object recognition. • SD- diagnosed with loss of comprehension of word meaning, object identity, or face identity. • bvFTD- diagnosed with personality and behavioral changes significant enough to interfere with work or interpersonal relationships, and at least 5 core symptoms of the disease.
Cognitive Instruments All participants were administered a standard neuropsychologic test battery consisting of these tests: • California Verbal Learning Test Free Recall • Number Cancellation • Digits Backward from Wechsler Memory Scale-Revised • Stroop Test • Digit-Symbol Substitution • Verbal Fluency for Letters and Categories • Boston Naming Test All tests were scored by board certified behavioral neurologists. Tests were chosen based on Knopman et al., 2008.
Computerized Psycholinguistic Assessments • natural language processing (NLP) and automatic speech recognition (ASR)—a set of computational techniques used for computerized analysis of speech and language. The use of ASR and NLP to psychometric testing is new; however it was felt by the researchers of this study to be a natural extension of the capabilities of this technology. For this study, a system for semiautomated language and speech analysis based on NLP and ASR technology. The system was configured for this study to process audio recordings of speech elicited during the Cookie-Theft picture description task of the Boston Diagnostic Aphasia Examination. Audio input was manually transcribed and then aligned with the transcribed text. (Refer to Appendix A of the study).