Download
1 / 49
581 likes | 1.87k Views
Note this is at basic level for 2nd year medical students & Allied Health students.

E N D
Pathology of WBC Disorders Aspire to become good, not great....Greatness is like a passing cloud,temporary.- Sai Baba - Divine Discourse, July 16, 2001.
Pathology ofWBC disordersDr. Shashidhar Venkatesh MurthyA/Prof. & Head of Pathology2013: MB2-HRM-Week 7 Pathology ofWBC disordersDr. Shashidhar Venkatesh MurthyA/Prof. & Head of Pathology2013: MB2-HRM-Week 7
HRM-Wk7: Fever, bleeding & Back pain Mr M.S. 45y, man. Presents to ED: “Verybad lower back pain, nothing helping it”. History:• Feels unwell? - Very• Fever? Yes, I think so; intermittent• Easy bruising -Yes, bruises last few weeks. Examination:• Slim, unwell, pale, Multiple Bruises• Liver & Spleen enlarged – mild.• Lymph nodes enlarged neck & axilla. HRM-Wk7: Fever, bleeding & Back pain Mr M.S. 45y, man. Presents to ED: “Verybad lower back pain, nothing helping it”. History:• Feels unwell? - Very• Fever? Yes, I think so; intermittent• Easy bruising -Yes, bruises last few weeks. Examination:• Slim, unwell, pale, Multiple Bruises• Liver & Spleen enlarged – mild.• Lymph nodes enlarged neck & axilla.
Learning Objectives: WBC in health & disease - overview. Classification & Common WBC disorders. Congenital, Reactive & Cancer. Clinical features. Pathogenesis Laboratory diagnosis Blood morphology• Features (3-4).• Line diagram. Management - brief.TOP 10 WBC Disorders:• Leukopenia:1. Neutropenia2. Lymphopenia.3. Pancytopenia• Leucocytosis:4. Neutrophilia5. Eosinophilia6. Lymphocytosis – IM7. Lymphadenitis.• Neoplastic disorders (cancer)9. Lymphoma10. Leukemia (AML/ALL,CML/CLL) Learning Objectives: WBC in health & disease - overview. Classification & Common WBC disorders. Congenital, Reactive & Cancer. Clinical features. Pathogenesis Laboratory diagnosis Blood morphology• Features (3-4).• Line diagram. Management - brief.TOP 10 WBC Disorders:• Leukopenia:1. Neutropenia2. Lymphopenia.3. Pancytopenia• Leucocytosis:4. Neutrophilia5. Eosinophilia6. Lymphocytosis – IM7. Lymphadenitis.• Neoplastic disorders (cancer)9. Lymphoma10. Leukemia (AML/ALL,CML/CLL)
Teaching Plan & Staff: Introduction to WBC disorders:• Shashidhar Venkatesh Murthy. Clinical Cases: GLS 1st hour.• Ian Irving, Haematologist, TSVH. Microscopy Tutorial: GLS 2nd hour.• Shashidhar Venkatesh Murthy. Synthesis Session: Keepad Q&A disc.• Shashidhar Venkatesh Murthy.Mon9amTue1pmTue2pmThu1pm Teaching Plan & Staff: Introduction to WBC disorders:• Shashidhar Venkatesh Murthy. Clinical Cases: GLS 1st hour.• Ian Irving, Haematologist, TSVH. Microscopy Tutorial: GLS 2nd hour.• Shashidhar Venkatesh Murthy. Synthesis Session: Keepad Q&A disc.• Shashidhar Venkatesh Murthy.Mon9amTue1pmTue2pmThu1pm
8y child with Asthma & multiple scaly skin lesions.Image shows blood film appearance. ? Cause1. Viral Infection2. Allergic reaction3. Malaria.4. Bacterial infection.5. Fungal infection.1 2 3 4 50 0 000SYNTHESIS SESSION 8y child with Asthma & multiple scaly skin lesions.Image shows blood film appearance. ? Cause1. Viral Infection2. Allergic reaction3. Malaria.4. Bacterial infection.5. Fungal infection.1 2 3 4 50 0 000SYNTHESIS SESSION
I am here for you….Email: venkatesh.shashidhar@jcu.edu.auvmshashi@gmail.comNeed personal guidance? Email me for an appointment.Office Tel: 4781 4566Office location – MS136Emergency?(exam time) Mob: 0416 933 704 I am here for you….Email: venkatesh.shashidhar@jcu.edu.auvmshashi@gmail.comNeed personal guidance? Email me for an appointment.Office Tel: 4781 4566Office location – MS136Emergency?(exam time) Mob: 0416 933 704
Small minds discuss peopleAverage minds discuss eventsGreat minds discuss solutionGenius silently acts! Small minds discuss peopleAverage minds discuss eventsGreat minds discuss solutionGenius silently acts!
. 10Normal Blood Cells:NeutrophilBasophilEosinophilLymphocyteNon granular, MononuclearsSpecific ImmunityGranulocytes, PolymorphsNon-Specific Immunity
. Normal Granulopoiesis: CSFStimulatebone marrowto produceWBC.What are the Clinical applications of G-CSF?
. Lab: CBC - WBC Histogram:AbsoluteCount% / Differential Count
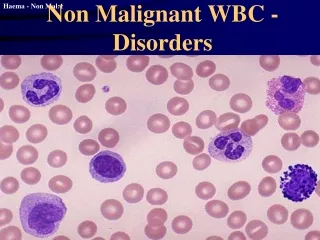
. WBC Absolute counts in disease:Penia PhiliaNeutroPenia PhiliaEosinoPenia cytosisMonoPenia cytosisLympho
. Leukopenia: Neutropenia Reduction in granulocytes:• Decreased Production – Marrow.• Increased destruction – drugs, immune When severe – Agranulocytosis. Clinical features:• Infections – chills, fever, fatigue, ulcers.
. Leukocytosis: Neutrophilia Increased granulocytes:• Acute inflammation, Bacterial infections. When severe – Leukemoid reaction. Clinical features:• Infections or Trauma - fever, fatigue.
. Lymphocytosis: Infectious Mononucleosis Increased Lymphocytes:• Chronic Inflam, Viral, fungal, TB etc. Large lymphocytes, more cytoplasm. Irregular,indented by RBC – also known as virocyte Clinical features: Chronic fever, lymphadenopathy.
. Neutrophilia:Acute inflammation (Bacterial, trauma, immune, etc)
. Toxic Granulation & Left shift:Acute inflammation Bacterial, trauma, immune, etcBand forms & Phagocytic granules in cytoplasm
. Leukemoid Reaction: Marked increase inneutrophils. >50,000 x109 Shift to left immatureforms. Severe infection, trauma,bone marrow infiltration. Looks like leukemia*(no blasts)
. Your failure may prove to bean asset, provided you try toknow why you failed !--Napoleon Hill
. Lymphadenitis: Reactive. Acute or Chronic. Infections, Immune & Cancers. Increased large irregular lymphoid follicleswith normal archetecture. (mantle zone). Lymphadenitis: Enlarged lymphnodes dueto inflammation or infecitons. Painful. Lymphadenopathy – any enlargement, butcommonly used for Cancers – Painless.
. Reactive lymphadenitisDark zoneLight zoneMantle zoneMacrophageTingible bodyMacrophage
. Hemato-oncology: Blood Cancer Cancer of blood forming – stem cells (Blasts). Leukemia – ‘White’ ‘blood’ – excess WBC. Starts in bone marrow or lymphatic tissue. Spread to blood & other ‘RES’ tissues only.(Liver, Spleen & lymphnodes) Two Major types: Myeloid & Lymphoid. Two clinical presentaiton: Acute / Chronic. Many subtypes* – due to several differentmutations – personalized medicine *
. The goal of mankind is knowledge, whichis inherent in man. No knowledge comesfrom outside: it is all inside. What manlearns is really what he “discovers” bytaking the cover off his own soul.- - Swami Vivekananda„Education‟… from Eduse (latin) to bring out..!„Doctor‟ … from Dokere‟ (latin) to teach…!
. LymphoblastLeukemia: Cancer of Blast cells.AcuteMyeloidLeukemiaAcute Lymphatic LeukemiaChronic LeukemiaChronic Leukemia
. Normal – Acute - Chronic LeukNormalChronic Myeloid LeukemiaAcute Myeloid Leukemia
. Hematologic Neoplasms: Classification Leukemias: Bone marrow, blood, Blasts• Duration: Acute/Chronic• Cell of Origin: Myeloid/Lymphoid• AML / ALL & CML / CLL Lymphomas: – Lymph nodes, tumor• Hodgkins & Non-Hodgkins. Premalignant conditions:• Myeloproliferative syndromes (MPS)• Myelodysplastic syndromes (MDS)
. Leukemia: Clinical Features Cancer of Bone marrow – Excess blasts. Decreased Haemopoiesis:• Erythropoiesis – Anemia - RBC• Leukopoiesis – Infections - WBC• Thrombopoiesis – Bleeding. PLT Bone marrow expansion/destruction:• Bone pains. Extraneous hemopoiesis / spread:• Splenomegaly• Hepatomegaly• Lymphadenopathy. (more in lymphatic malignancy)
. Leukemia Clinical features:Bleeding - PetechiaeLymphadenopathyHepatosplenomegalyInfections - Candidiasis
. Leukemia Classification Acute Leukemias: weeks to months.• Acute Myeloid Leukemia – AML - Adults• Many Subtypes: M0, M1 to M7• Acute Lymphoid Leukemia – ALL - Children• Many Subtypes: L1, L2 & L3 Chronic Leukemias: Years.• Chronic Myeloid Leukemia- CML- Adults• Chronic Lymphoid Leukemia - CLL –Old age• Many subtypes:
. Acute Leukemia: AML/ALL - BlastsNorm. LymphocyteBlastBlastNorm. RBCNorm. LymphocyteNorm. RBCBlastNormal
. Lymphoma Definition: Tumour of lymphoid tissue Etiology: Idiopathic, Genetic, Infective. Clinical: Lymphadenopathy, weight loss, Fever. Two Major Types: & many subtypes. Hodgkins lymphoma (HL) – RS cells. Non-Hodgkins lymphoma (NHL) – no RS cells.• B cell, T cell & Histiocytic lymphoma.
. Hodgkins LymphomaBig binucleate cancer cells known asReed Sternberg Cells (RS cells)
. Non-Hodgkins Lymphoma: Large group of lymphatic neoplasms. Clinical: Fever, anemia, infections,Lymphadenopathy. Spleen+/-. No RS cells or eosinophilia Complex names and classification.• Cell type – B, T & Histiocytic “B commonest”• Clinical – low, intermediate & high grade.• Histology – Follicular & diffuse.• Special types: Burkitts lymphoma, Myeloma,Waldenstroms macroglobulinemia, lennert‟s,
. Non Hodgkins LymphomaLow, Intermediate & High grade.
. Burkitt‟s lymphoma: large B cell NHL Endemic in Africa Epstein Barr Virus(EBV) B Cell Lymphoma. Dark large Blymphocytes (malignant)with plenty of palemacrophages. (Starrysky pattern).
. Multiple Myeloma: Malignancy of Plasma cells(Mature B lymph, Ab) Old age, males common. Marrow, LN, Blood. Multiple, punched out Lytic bonelesions (Osteolysis) Hyper gammaglobulinemia Monoclonal antibody peak –serum protein electrophoresis. Immunodeficiency infections.
. "Creativity is inventing,experimenting, growing, takingrisks, breaking rules, makingmistakes, and having fun.-- Mary Lou Cook
. Myeloproliferative Disorders.Myelodysplastic Syndromes.(Precanceraous stage of blood cancers)
. Myelo Proliferative Disorders: Excess Proliferation, Neoplastic, Old age. Organomegaly – Liver & Spleen enlarged. Hypercellular BM & Leukocytosis. 4 types:• Excess RBC (polycythemia vera)• Excess WBC (CML)• Excess Plt (Essential Thrombocythemia)• Excess Fibroblast (Myelofibrosis). Mixed types common, end in leukemia.
. Polycythemia Rubra Vera (PV)Hypercellular Marrow,Red skin & Hepatosplenomegaly
. ET - Blood Film & clinical.Plenty ofPlateletsMegakaryocyte
. Myelo Dysplastic Syndromes: Dysplastic Proliferation (abnormal cells) Neoplastic, old age, unexplained anemia. Abnormal cells destroyed in bone marrow. Hypercellular BM & Leukopenia, anemia. Commonly known as Refractory Anemia. Many subtypes, Mild to severe dysplasia. Increasing blasts – poor prognosis. Transforms to acute leukemia.
. Summary: Reactive Leukocytosis.• Neutrophilia, Eosinophilia, Lymphocytosis. Reactive Leukopenia.• Neutropenia, lymphopenia. Leukemias – Cancer of Blasts.• AML/ALL, CML/CLL Lymphomas – Tumors of lymphoid tissue• Hodgkins & Non- Hodgkins (HL, NHL) Premalignant conditions• MPS & MDS:
. 3 R’s of success:Respect for self,Respect for others &Responsibility for your actions.