Download
1 / 51
850 likes | 2.56k Views
HEAD GEAR. DR. ABDUL JABBAR. Means of applying posterior directed forces to teeth and skeletal structures from an extra oral source. Headgear Introduced in late 1800s Abandoned as it was thought that intra- oral elastics would be as effective

E N D
HEAD GEAR DR. ABDUL JABBAR
Means of applying posterior directed forces to teeth and skeletal structures from an extra oral source
Headgear • Introduced in late 1800s • Abandoned as it was thought that intra- oral elastics would be as effective • Reintroduced in 1940s after cephalometric developed
Mechanism of action • Growth modification by changing the pattern of bone apposition at the sutures • CL II correction is obtained as the mandible grows forward normally while maxillary growth is restrained • Favorable mandibular growth is a must for CL II correction with HG use
Force is generated by head cap or neck strap through ; • springs • Elastic bands
Force is delivered to the teeth by ; • Face bow • J Hooks
classification • Distalising HG: direction of elastic traction has a distal component Types : Occipital directed ( high) pull Combination pull Cervical directed (low) pull J-hook HG • Asymmetric HG • HG to mandible
High Pull Headgear Skeletal Class II with prognathic maxilla High Angle case Growing ages • Straight Pull Headgear Skeletal Class II with prognathic maxilla normal Angle case Growing ages • Cervical Pull Headgear Skeletal Class II with prognathic maxilla Low Angle case Growing ages
Single pull to maxillary dentition • Attachment of the J hooks to both maxillary and mandibular dental arches.
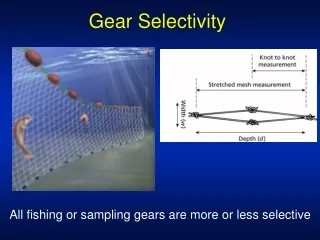
Components • Head cap / neck strap • Elastics • Face bow (Inner bow, outer bow and U loop)
Uses: dental • Anchorage • Distalisation – single or blocks of teeth • Intrusion -- single or blocks of teeth • Extrusion • Asymmetric movement
Uses: skeletal • growth modification • maxilla --- suppression which is permanent even after treatment has ceased • mandible --- suppression, retrusion of the chin during chin cap treatment.however catch-up mandibular growth may occur during or after pubertal growth period
Factors influencing effect • Direction of force • Duration of force • Magnitude of force • Centers of rotation
Duration and magnitude of force • Orthopedic effect • Principle: higher forces for comparatively smaller duration • 12 ---16 oz or 350-----450 gm / side • 10 ---12 hrs
Duration and magnitude of force • Tooth movement • Principle : smaller forces for longer duration • 100 --- 200 gm / side • 14 --- 16 hrs • Anchorage • 250 --- 300 gm / side • 10 hrs min.
Magnitude of force is determined by a Strain-gauge • Spring loaded assembly comes with a built-in force indicator
Centers of rotation Single rooted teeth ----- centroid 6_ ----- trifurcation Maxilla ----- b/w roots of 4&5
Resolution of forces:horizontally • Force thru center of resistance ----- bodily movement • Force above center of resistance ----- distal root tipping • Force below center of resistance ----- mesial root tipping
Resolution of forces:Vertically • Above occlusal plane ----- intrudes teeth • Below occlusal plane ----- extrudes teeth
Problems with HGTooth- related • Unwanted tooth movement • Tipping • Extrusion of 6_ may cause clockwise rotation of mand. Pt. Becomes more CLII • Buccal rolling of 6_ with high pull HG • Cross bite on side of movement with asymmetric HG • Lingual tipping of lower incisors, clockwise rotation of mand. & increased LAFH with chin cup therapy • Root resorption possibly with J hook HG
Problems with HGPatient related • Co-operation • biological variability growth may be unfavorable • Extra / intra-oral injuries • Pain • Difficulty with insertion
Assessment of patient compliance at every visit • Check for signs of use intra orally as well as extra orally • Hand out Time-sheets for record of wear • Offer reward
Extra oral injuries include injuries to eyes , eyelids, nose etc. • Most common are eye injuries • Catapult type of injury very common while playing • Disengagement of face bow during sleep
Safety • No single safety HG is best • Should use safety face bow and release mechanism together • Written instructions must be given to patient • Risks involved should be explained • told to seek medical advice if any problem arises