Download
1 / 1
10 likes | 134 Views
The Prognostic and Pathogenetic Significance of Severe Focal Segmental Lupus Glomerulonephritis Melvin M. Schwartz, MD, Stephen M. Korbet MD, MD, and Edmund J. Lewis MD Rush University Medical Center, Chicago, IL. Introduction. Materials and Methods Cont. Results Cont. Results Cont.

E N D
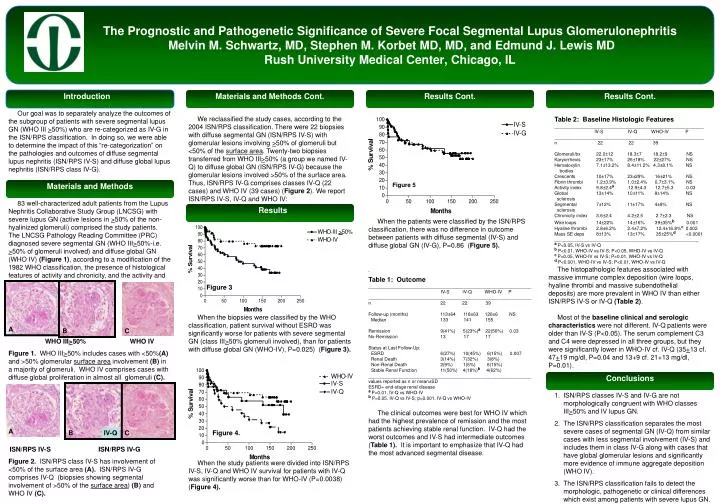
The Prognostic and Pathogenetic Significance of Severe Focal Segmental Lupus Glomerulonephritis Melvin M. Schwartz, MD, Stephen M. Korbet MD, MD, and Edmund J. Lewis MDRush University Medical Center, Chicago, IL Introduction Materials and Methods Cont. Results Cont. Results Cont. Our goal was to separately analyze the outcomes of the subgroup of patients with severe segmental lupus GN (WHO III >50%) who are re-categorized as IV-G in the ISN/RPS classification. In doing so, we were able to determine the impact of this “re-categorization” on the pathologies and outcomes of diffuse segmental lupus nephritis (ISN/RPS IV-S) and diffuse global lupus nephritis (ISN/RPS class IV-G). We reclassified the study cases, according to the 2004 ISN/RPS classification.There were 22 biopsies with diffuse segmental GN (ISN/RPS IV-S) with glomerular lesions involving >50% of glomeruli but <50% of the surface area. Twenty-two biopsies transferred from WHO III>50% (a group we named IV-Q) to diffuse global GN (ISN/RPS IV-G) because the glomerular lesions involved >50% ofthe surface area.Thus, ISN/RPS IV-G comprises classes IV-Q (22 cases) and WHO IV (39 cases) (Figure 2).We report ISN/RPS IV-S, IV-Q and WHO IV: Table 2: Baseline Histologic Features __________________________________________________________ IV-S IV-Q WHO-IV P __________________________________________________________ n 22 22 39 Glomeruli/bx 22.0±12 18.3±7 18.2±9 NS Karyorrhexis 23±17% 26±18% 22±27% NS Hematoxylin 7.1±13.2% 8.4±11.2% 4.3±8.1% NS bodies Crescents 10±17% 23±29% 16±21% NS Fibrin thrombi 1.2±3.9% 1.0±2.4% 0.7±3.1% NS Activity index 9.8±2.4a 12.9±4.3 12.7±5.3 0.03 Global 13±14% 10±11% 8±14% NS sclerosis Segmental 7±12% 11±17% 4±9% NS sclerosis Chronicity index 3.6±2.4 4.2±2.5 2.7±2.3 NS Wire loops 14±22% 14±16% 39±35%b 0.001 Hyaline thrombi 2.8±6.2% 2.4±7.2% 12.4±16.8%c 0.002 Mass SE deps 8±13% 13±17% 35±25%d<0.0001 ________________________________________________________ a P<0.05, IV-S vs IV-Q b P<0.01, WHO-IV vs IV-S; P<0.05, WHO-IV vs IV-Q c P<0.05, WHO-IV vs IV-S; P<0.01, WHO-IV vs IV-Q d P<0.001, WHO-IV vs IV-S; P<0.01, WHO-IV vs IV-Q Materials and Methods Figure 5 83 well-characterized adult patients from the Lupus Nephritis Collaborative Study Group (LNCSG)with severe lupus GN (active lesions in >50% of the non-hyalinized glomeruli)comprised the study patients. The LNCSG Pathology Reading Committee (PRC) diagnosed severe segmental GN (WHO III>50%-i.e. >50% of glomeruli involved) and diffuse global GN (WHO IV) (Figure 1), according to a modification of the 1982 WHO classification, the presence of histological features of activity and chronicity, and the activity and chronicity indices. Results When the patients were classified by the ISN/RPS classification, there was no difference in outcome between patients with diffuse segmental (IV-S) and diffuse global GN (IV-G), P=0.86 (Figure 5). The histopathologic features associated with massive immune complex deposition (wire loops, hyaline thrombi and massive subendothelial deposits) are more prevalent in WHO IV than either ISN/RPS IV-S or IV-Q (Table 2). ‘ Table 1: Outcome _______________________________________________________________ IV-S IV-Q WHO-IV P _______________________________________________________________ n 22 22 39 Follow-up (months) 113±64 118±63 126±6 NS Median 133 141 155 Remission 9(41%) 5(23%)a 22(56%) 0.03 No-Remission 13 17 17 Status at Last Follow-Up: ESRD 6(27%) 10(45%) 6(15%) 0.007 Renal Death 3(14%) 7(32%) 3(8%) Non-Renal Death 2(9%) 1(5%) 6(15%) Stable Renal Function 11(50%) 4(18%)b 4(62%) _______________________________________________________________ values reported as n or mean±SD ESRD= end-stage renal disease a P=0.01, IV-Q vs WHO-IV b P=0.05, IV-Q vs IV-S; p=0.001, IV-Q vs WHO-IV Figure 3 When the biopsies were classified by the WHO classification, patient survival without ESRD was significantly worse for patients with severe segmental GN (class III>50% glomeruli involved), than for patients with diffuse global GN (WHO-IV), P=0.025) (Figure 3). Most of the baseline clinical and serologic characteristics were not different. IV-Q patients were older than IV-S (P<0.05). The serum complement C3 and C4 were depressed in all three groups, but they were significantly lower in WHO-IV cf. IV-Q (35+13 cf. 47+19 mg/dl, P=0.04 and 13+9 cf. 21+13 mg/dl, P=0.01). A A B C WHO III>50% WHO IV Figure 1. WHO III>50% includes cases with <50%(A) and >50% glomerular surface area involvement (B) in a majority of glomeruli. WHO IV comprises cases with diffuse global proliferation in almost all glomeruli (C). Conclusions • ISN/RPS classes IV-S and IV-G are not morphologically congruent with WHO classes III>50% and IV lupus GN. • The ISN/RPS classification separates the most severe cases of segmental GN (IV-Q) from similar cases with less segmental involvement (IV-S) and includes them in class IV-G along with cases that have global glomerular lesions and significantly more evidence of immune aggregate deposition (WHO IV). • The ISN/RPS classification fails to detect the morphologic, pathogenetic or clinical differences which exist among patients with severe lupus GN. The clinical outcomes were best for WHO IV which had the highest prevalence of remission and the most patients achieving stable renal function. IV-Q had the worst outcomes and IV-S had intermediate outcomes (Table 1). It is important to emphasize that IV-Q had the most advanced segmental disease. A B IV-Q C Figure 4. Results ISN/RPS IV-S ISN/RPS IV-G Figure 2. ISN/RPS class IV-S has involvement of <50% of the surface area (A). ISN/RPS IV-G comprises IV-Q (biopsies showing segmental involvement of >50% of the surface area) (B) and WHO IV (C). When the study patients were divided into ISN/RPS IV-S, IV-Q and WHO IV survival for patients with IV-Q was significantly worse than for WHO-IV (P=0.0038) (Figure 4).






















