Download
1 / 63
630 likes | 741 Views
Carpal Tunnel Syndrome. Stacey Harris-Carriman, M.D. Physical Medicine and Rehabilitation Noon Conference, CCRMC May 8, 2009. Objectives. Be familiar with the basic neuroanatomy of the upper limb Understand factors involved in diagnosing CTS Recognize the goals and limitations of NCS

E N D
Carpal Tunnel Syndrome Stacey Harris-Carriman, M.D. Physical Medicine and Rehabilitation Noon Conference, CCRMC May 8, 2009
Objectives • Be familiar with the basic neuroanatomy of the upper limb • Understand factors involved in diagnosing CTS • Recognize the goals and limitations of NCS • Review treatment of CTS
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
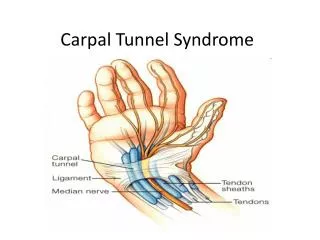
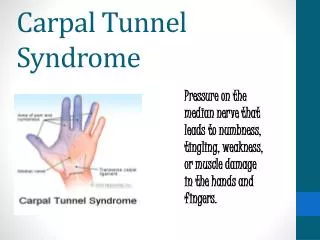
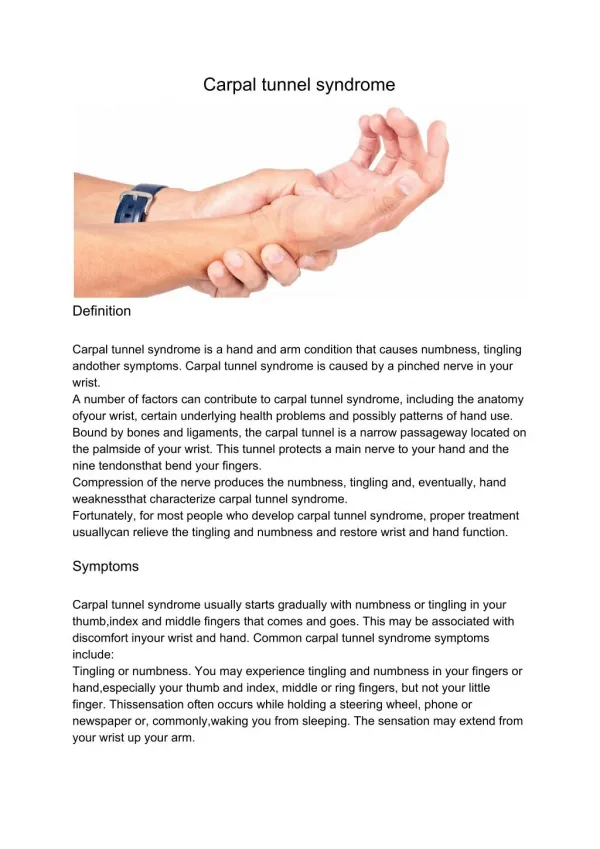
Constellation of symptoms and signs secondary to a median neuropathy at the wrist Definition of CTS
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
Etiology • Majority of CTS cases idiopathic
Small percentage of CTS due to an identifiable cause, such as: DM, RA, thyroid disease Conditions that increase total body fluid (e.g. pregnancy, hemodialysis) Local wrist lesion (e.g. cyst, fracture, infection, tumor) Congenital (e.g. small carpal tunnel) Etiology
Risk Factors • Gender: F 3x>M • Age: • Older > younger; very rare in children • Peak prevalence in women >55
Family history Certain medical conditions Workers that use hands and wrists repetitively, especially with high force Musicians Risk Factors
Risk Factors • Other: Smoking, alcohol, poor nutrition, obesity, high cholesterol
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
Symptoms • Pattern recognition • Wide variety of symptoms in CTS • Some symptoms are more suggestive of CTS than other symptoms
Symptoms • Classic symptoms in CTS: • Waking up with pain and numbness/paresthesias of the hand • Triggered by driving, holding phone, reading book, typing, writing • Relieving factors • Flick sign • Changes in hand posture
Signs • Key signs suggestive of CTS • Impaired sensation of the lateral 3-1/2 digits • Weakness of APB and other median-innervated muscles of thenar eminence • Phalen’s, reverse Phalen’s • Tinel’s • Other: Pressure provocation test, hand elevation test, tourniquet test
Signs NOT consistent with CTS • Impaired sensation over the lateral palm (thenar region) • Impaired sensation proximal to wrist • Weakness of hypothenar muscles or other non-median-innervated muscles • Impaired deep tendon reflexes
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
Peripheral NS Cervical radiculopathy Brachial plexopathy Proximal median neuropathy (e.g. in forearm or elbow) Other mononeuroapthy (e.g. ulnar, radial) Underlying polyneuropathy Central NS (e.g. TIA, small lacunar infarct, myelopathy) Musculoskeletal Shoulder pain with distal paresthesias Osteoarthritis Cumulative trauma disorder Differential Diagnosis of CTS
Peripheral NS: Cervical radiculopathy Differential Diagnosis
Especially mild cases of cervical radiculopathy C6, C7 Neck pain, radiation to shoulder, arm, +/- distally Worse with neck movement Impaired reflexes and strength Sensory loss beyond distribution of median nerve DDx: Cervical Radiculopathy
Peripheral NS: Brachial Plexopathy Differential Diagnosis
Uncommon Etiology: Trauma Tumor, Mass Delayed radiation injury Plexitis Postop (e.g. CABG) Neurogenic TOS DDx: Brachial Plexopathy
DDx: Brachial Plexopathy • Trauma • Most common cause of brachial plexopathy • Mechanism: • Traction • Car/motorcycle/bike accident, newborn • Upper trunk C5/6-Erb’s palsy • Lower trunk C8/T1-Klumpke’s palsy • Penetrating (knife, bullet)
DDx: Brachial Plexopathy • Neoplasm, Mass • Metastasis to lymph nodes (most common), especially lymphoma, breast, lung cancer • Local tumor: Pancoast • Other • Direct infilration of nerve: Lymphoma, leukemia • Rare: Primary nerve sheath tumor • Non-neoplastic (unusual): hematoma, vascular anomaly
Delayed Radiation VS Onset: Progressive, years after radiation Risk correlated with dose of radiation Sensory sx prominent (paresthesias, numbness) (Recurrent) Neoplasm Onset: Slowly progressive Prominent pain Horner’s syndrome DDx: Brachial Plexopathy
Brachial Plexitis AKA Neuralgic amyotrophy, Parsonage-Turner Idiopathic Often preceded by: viral illness or immunization; also surgery Long thoracic nerve, anterior interosseous nerve, other Shoulder pain Onset: days to weeks after inciting event Severe pain, awakens from sleep Weakness and atrophy Onset: Generally after pain subsides (1-2 weeks) +/- Sensory s/sx DDx: Brachial Plexopathy
Neurogenic TOS Most cases due to fibrous band between cervical rib and 1st thoracic rib Lower trunk, C8/T1 Exam: Muscles: hand intrinsics, esp thenar T1; +/- FPL, FDP Sensory: Ulnar, MABC DDx: Brachial Plexopathy
Peripheral NS: Proximal Median Neuropathy Differential Diagnosis
Rare Trauma Ligament of Struthers Anterior Interosseous Syndrome Pure motor: FPL, PQ, FDP to #2-3 “Okay” sign “Pronator Syndrome” Possible sites of entrapment Pronator teres Lacertus fibrosus (b/t biceps tendon and proximal flexor forearm muscles) Aponeurotic ridge of FDS (sublimis bridge) DDx: Proximal Median Neuropathy
Differential Diagnosis • Peripheral NS: Other Mononeuropathy • Ulnar, Radial
Peripheral NS: Peripheral Polyneuropathy Differential Diagnosis
CNS: Cervical Myelopathy Differential Diagnosis
Musculoskeletal: Shoulder Pathology with Distal Paresthesias Differential Diagnosis
Outline • Definition • Etiology and Risk Factors • Neuroanatomy of the Upper Limb • Diagnosis: Symptoms and signs • Differential diagnosis • NCS/EMG and US • Treatment
Nerve Conduction Studies (NCS) • [NOTE: NCS sometimes called NCV “Nerve Conduction Velocity”]
NCS • Picture here of NCS set-up
NCS • NCS can be useful in confirming CTS and assessingseverity of CTS
NCS • An extension of the clinical examination • Each NCS study must be individualized
NCS • NCS is positive in 91-98% of patients with clinically diagnosed CTS • (Source: Keles et al, Diagnostic precision of ultrasonography in patients with CTS, Am J Phys Med Rehabil 2005) • Risk of false negatives on NCS generally implies very mild CTS
Diagnostic Ultrasound • Real-time imaging of median nerve in carpal tunnel • Qualitative and quantitative • Measurements can include: • Cross-sectional area (CSA) of median nerve • Bowing of flexor retinaculum • Flattening of median nerve in carpal tunnel
Diagnostic Ultrasound • Relatively new development • Aids in diagnosis • Aids in treatment, ultrasound-guided injection of steroid into carpal tunnel