Download
1 / 1
10 likes | 174 Views
Endoscopic Ultrasound Directed Pseudocyst Drainage without the use of Fluoroscopy: A Case Series Abdalla, Maisa MD. 1 ; Majmundar, Kaeya 1 ; Berkelhammer , Charles MD. 1 ; Gamagami, Reza MD. 3 ; Blumenstein, Brian MD. 1 ; Carter, Yvonne RN. 1 ; Ayub, Kamran MD 1, 2,3

E N D
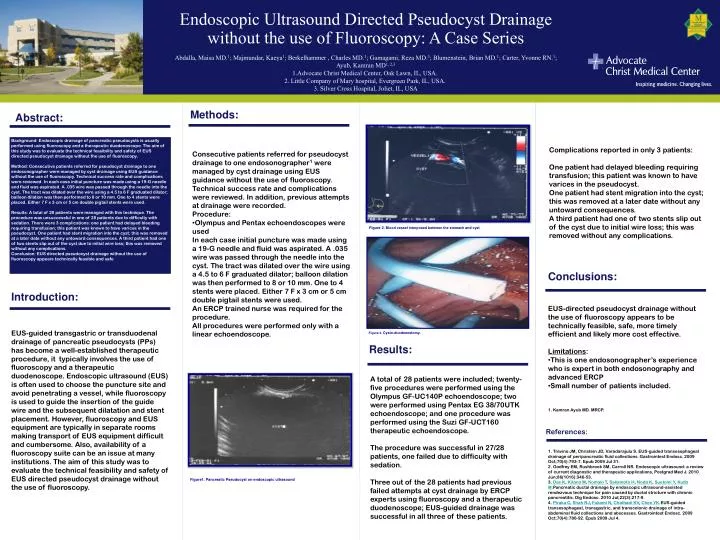
Endoscopic Ultrasound Directed Pseudocyst Drainage without the use of Fluoroscopy: A Case Series • Abdalla, Maisa MD.1; Majmundar, Kaeya1; Berkelhammer , Charles MD.1; Gamagami, Reza MD.3; Blumenstein, Brian MD.1; Carter, Yvonne RN.1; Ayub, Kamran MD1, 2,3 • Advocate Christ Medical Center, Oak Lawn, IL, USA. • 2. Little Company of Mary hospital, Evergreen Park, IL, USA. • 3. Silver Cross Hospital, Joliet, IL, USA Methods: Abstract: Background: Endoscopic drainage of pancreatic pseudocysts is usually performed using fluoroscopy and a therapeutic duodenoscope. The aim of this study was to evaluate the technical feasibility and safety of EUS directed pseudocyst drainage without the use of fluoroscopy. Method: Consecutive patients referred for pseudocyst drainage to one endosonographer were managed by cyst drainage using EUS guidance without the use of fluoroscopy. Technical success rate and complications were reviewed. In each case initial puncture was made using a 19-G needle and fluid was aspirated. A .035 wire was passed through the needle into the cyst. The tract was dilated over the wire using a 4.5 to 6 F graduated dilator; balloon dilation was then performed to 8 or 10 mm. One to 4 stents were placed. Either 7 F x 3 cm or 5 cm double pigtail stents were used. Results: A total of 28 patients were managed with this technique. The procedure was unsuccessful in one of 28 patients due to difficulty with sedation. There were 3 complications: one patient had delayed bleeding requiring transfusion; this patient was known to have varices in the pseudocyst. One patient had stent migration into the cyst; this was removed at a later date without any untoward consequences. A third patient had one of two stents slip out of the cyst due to initial wire loss; this was removed without any complications. Conclusion: EUS directed pseudocyst drainage without the use of fluoroscopy appears technically feasible and safe Complications reported in only 3 patients: One patient had delayed bleeding requiring transfusion; this patient was known to have varices in the pseudocyst. One patient had stent migration into the cyst; this was removed at a later date without any untoward consequences. A third patient had one of two stents slip out of the cyst due to initial wire loss; this was removed without any complications. • Consecutive patients referred for pseudocyst drainage to one endosonographer1 were managed by cyst drainage using EUS guidance without the use of fluoroscopy. Technical success rate and complications were reviewed. In addition, previous attempts at drainage were recorded. • Procedure: • Olympus and Pentax echoendoscopes were used • In each case initial puncture was made using a 19-G needle and fluid was aspirated. A .035 wire was passed through the needle into the cyst. The tract was dilated over the wire using a 4.5 to 6 F graduated dilator; balloon dilation was then performed to 8 or 10 mm. One to 4 stents were placed. Either 7 F x 3 cm or 5 cm double pigtail stents were used. • An ERCP trained nurse was required for the procedure. • All procedures were performed only with a linear echoendoscope. Figure 2. Blood vessel interposed between the stomach and cyst Conclusions: Introduction: • EUS-directed pseudocyst drainage without the use of fluoroscopy appears to be technically feasible, safe, more timely efficient and likely more cost effective. • Limitations: • This is one endosonographer’s experience who is expert in both endosonography and advanced ERCP • Small number of patients included. EUS-guided transgastric or transduodenal drainage of pancreatic pseudocysts (PPs) has become a well-established therapeutic procedure, it typically involves the use of fluoroscopy and a therapeutic duodenoscope. Endoscopic ultrasound (EUS) is often used to choose the puncture site and avoid penetrating a vessel, while fluoroscopy is used to guide the insertion of the guide wire and the subsequent dilatation and stent placement. However, fluoroscopy and EUS equipment are typically in separate rooms making transport of EUS equipment difficult and cumbersome. Also, availability of a fluoroscopy suite can be an issue at many institutions. The aim of this study was to evaluate the technical feasibility and safety of EUS directed pseudocyst drainage without the use of fluoroscopy. Figure 3. Cysto-duodenostomy. Results: A total of 28 patients were included; twenty-five procedures were performed using the Olympus GF-UC140P echoendoscope; two were performed using Pentax EG 38/70UTK echoendoscope; and one procedure was performed using the Suzi GF-UCT160 therapeutic echoendoscope. The procedure was successful in 27/28 patients, one failed due to difficulty with sedation. Three out of the 28 patients had previous failed attempts at cyst drainage by ERCP experts using fluoroscopy and a therapeutic duodenoscope; EUS-guided drainage was successful in all three of these patients. 1. Kamran Ayub MD. MRCP. References: 1. Trevino JM, Christein JD, Varadarajulu S. EUS-guided transesophageal drainage of peripancreatic fluid collections. Gastrointest Endosc. 2009 Oct;70(4):793-7. Epub 2009 Jul 31. 2. Godfrey EM, Rushbrook SM, Carroll NR. Endoscopic ultrasound: a review of current diagnostic and therapeutic applications, Postgrad Med J. 2010 Jun;86(1016):346-53. 3. Das K, Kitano M, Komaki T, Sakamoto H, Noda K, Suetomi Y, Kudo M.Pancreatic ductal drainage by endoscopic ultrasound-assisted rendezvous technique for pain caused by ductal stricture with chronic pancreatitis. Dig Endosc. 2010 Jul;22(3):217-9. 4. Piraka C, Shah RJ, Fukami N, Chathadi KV, Chen YK.EUS-guided transesophageal, transgastric, and transcolonic drainage of intra-abdominal fluid collections and abscesses. Gastrointest Endosc. 2009 Oct;70(4):786-92. Epub 2009 Jul 4. Figure1. Pancreatic Pseudocyst on endoscopic ultrasound