Download
1 / 50
530 likes | 1.03k Views
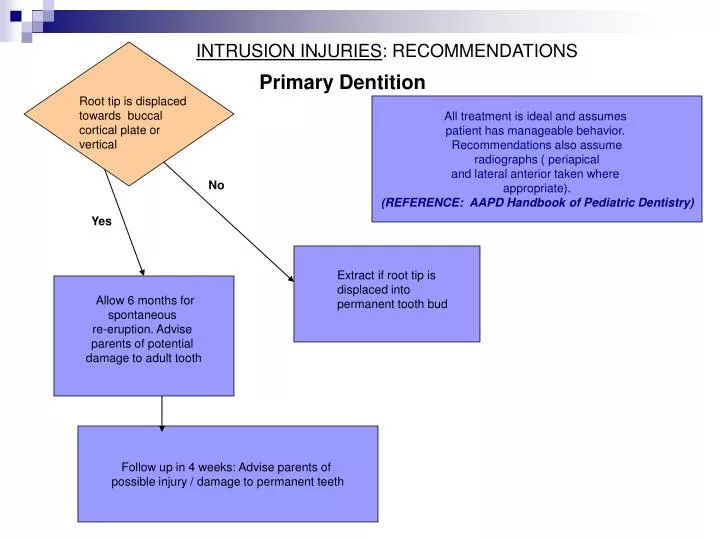
INTRUSION INJURIES : RECOMMENDATIONS. Primary Dentition. Root tip is displaced towards buccal cortical plate or vertical. All treatment is ideal and assumes patient has manageable behavior. Recommendations also assume radiographs ( periapical and lateral anterior taken where

E N D
INTRUSION INJURIES: RECOMMENDATIONS Primary Dentition Root tip is displaced towards buccal cortical plate or vertical All treatment is ideal and assumes patient has manageable behavior. Recommendations also assume radiographs ( periapical and lateral anterior taken where appropriate). (REFERENCE: AAPD Handbook of Pediatric Dentistry) No Yes Extract if root tip is displaced into permanent tooth bud Allow 6 months for spontaneous re-eruption. Advise parents of potential damage to adult tooth Follow up in 4 weeks: Advise parents of possible injury / damage to permanent teeth
Intrusive Luxation • Most common in upper primary incisors • Management: allow to re-erupt or extract
Tooth Not Retrieved Post Trauma • Confirm Intrusion with Periapical • Monitor up to 6 months for re-eruption
Intrusive LuxationPrimary Teeth • Consider antibiotic therapy - monitor for infection • Tetanus immunization current? • Extract if there are signs of swelling, spontaneous bleeding, abscess and fever Day of the Trauma 2 weeks Post Trauma
Intrusive LuxationPrimary Teeth • One of the most dangerous injuries to the developing tooth bud • Management: Minimize damage by assessing displacement of permanent bud
Ideally, a lateral film should be taken to confirm that intruded tooth has not displaced permanent tooth bud. If so, extraction recommended
Lateral Anterior Radiograph for Intruded Primary Tooth • Angulation of intruded tooth • Occlusal or size 4 extraoral film next to child’s cheek and perpendicular to radiographic beam • Exposure time is doubled
Intrusion Luxation: Re-eruption of Primary Tooth 2 months after injury 3 months after injury 1 year after injury
ROOT FRACTURES : RECOMMENDATIONS Primary Dentition All treatment is ideal and assumes patient has manageable behavior. Recommendations also assume appropriate pre-operative radiographs. (Source: AAPD Handbook of Pediatric Dentistry) Fracture located in coronal 1/3 of root or segment is aspiration risk Yes Extract coronal segment. Leave apical segment if not visible/easily removed No Clinical and radiographic follow up in 4 weeks: Advise parents of possible injury / damage to permanent teeth. NO SPLINT IS INDICATED
Root FracturesPrimary Teeth • Radiograph • Apical 1/3 - Most teeth maintain vitality and are minimally mobile - Apical fragment should resorb normally - Monitor with radiographs
Root FracturesPrimary Teeth • Radiograph • Middle or Cervical 1/3 - Most teeth mobile. Extraction indicated - Gently attempt to retrieve apical fragment If not successful, monitor - Don’t disrupt permanent tooth bud
Avulsion: Primary Teeth • Radiograph • Do not re-implant! • Space loss may not occur if primary canines are present • Permanent tooth eruption may be delayed due to scar tissue/bone
Parents Question: Will the permanent teeth be damaged? • May not be able to be determined until the teeth erupt and can be evaluated clinically • The accident has happened - we can’t reverse it • Monitor clinically and radiographically
Complications of Trauma • Permanent teeth malformation: • hypomineralization • hypoplasia • dilaceration • arrested development
History of Intrusive LuxationPrimary Teeth • Hypomaturation/Hypomineralization #8
History of Intrusion Luxation of Primary Tooth • Severe dilaceration of Root
History of Avulsion #E :Prior to Eruption of Primary Canines • Space maintainer not possible for pre-coop tot with incisors only • Ortho/space regaining will be needed
Acknowledgements • Photos and Diagrams taken from: • Textbook and Color Atlas of TraumaticInjuries to the Teeth, 4th edition: J.O. Andreasen (2007) • Pediatric Dentistry, 4th edition; Pinkham (2005) • Odontologia Para o Bebe’: Walter L.R.F. (1996) • University of Iowa, Department of Pediatric Dentistry
Competency Exam Answer the following questions on your worksheets
Case #1 “Anna” • Anna is a 4 y.o. girl who fell against the edge of a table about 2 hours ago • Her mother has given her children’s Tylenol and is at your office for evaluation • The upper incisors are tender, but non-mobile. • Her mother raises her lip to show you a 2 mm tear in the labial frenum area • Anna is cooperative
Case #1: “Anna” • What other clinical procedures do you need to perform? List at least 3.
“Anna’s” Pedo Occlusal • Is this radiograph within normal limits, or do you see any abnormalities or pathology?
Case #1 “Anna” • What is your plan for treatment and followup care for Anna? • What are your care instructions for mother?
Case #2: “Bart” • Bart is a 2 y.o. boy who fell against the edge of the bathtub about 1 hour ago • Mother felt his tooth “completely broke off at the gumline”, but could not find the piece • Clinically there are no additional findings
“Bart” • What radiographs are indicated for Bart?
Pedo Occlusal for “Bart” • Bart was not cooperative for further radiographs. What is your diagnosis based on this film?
Case #2 “Bart” • What is your plan for treatment and followup care?
Case #3: “Charlie” • Charlie is a healthy 3 y.o. boy who fell against the fireplace at home this morning • His father is with him • Clinical exam reveals enamel fracture #E and dentin fracture #F • No excessive mobility, no luxation • Occlusion is normal • Charlie is cooperative , but impatient and wiggly
Charlie’s Clinical Appearance (photo is a representation of the injury, not an actual photo of this patient) • What radiographs would you order for Charlie?
Case #3 “Charlie” • What is your plan for treatment and followup care for Charlie?
Case #4 “Davonne” • Davonne is a 12 year old boy with a non-contributory Health History • He and his parents are at your office for comprehensive care. • The chief complaint is “discolored lower front teeth.”
Davonne • What most likely caused this discoloration? • What are treatment options?
Competency Exam Answer Discussion
Case #1 “Anna” • Anna is a 4 y.o. girl who fell against the edge of a table about 2 hours ago • Her mother has given her children’s Tylenol and is at your office for evaluation • The upper incisors are tender, but non-mobile. • Her mother raises her lip to show you a 2 mm tear in the labial frenum area • Anna is cooperative
Case #1: “Anna” • What other clinical procedures do you need to perform? List at least 3. • Periapical radiograph (pedo occlusal) • Mobility check • Percussion check • Occlusion check • Complete hard and soft tissue assessment
“Anna’s” Pedo Occlusal • Is this radiograph within normal limits, or do you see any abnormalities or pathology? Answer: Within Normal Limits
Case #1 “Anna” • What is your plan for treatment and followup care for Anna? • Do not suture • Observe clinically and radiographically • What are your care instructions for mother? • OTC pain meds prn • Soft diet for about 1 week • Tooth may discolor, but this may reverse • Periodic reassessment needed
Case #2: “Bart” • Bart is a 2 y.o. boy who fell against the edge of the bathtub about 1 hour ago • Mother felt his tooth “completely broke off at the gumline”, but could not find the piece • Clinically there are no additional findings
“Bart” • What radiographs are indicated for Bart? • Periapical (pedo occlusal) • Lateral
Pedo Occlusal for “Bart” • Bart was not cooperative for further radiographs. What is your diagnosis based on this film? • Intrusion. No fracture detected.
Case #2 “Bart” • What is your plan for treatment and followup care? • Monitor for re-eruption • Consider antibiotic therapy and assess tetanus immunization • Explain signs and symptoms of infection. • Re-assess in 2 weeks
Case #3: “Charlie” • Charlie is a healthy 3 y.o. boy who fell against the fireplace at home this morning • His father is with him • Clinical exam reveals enamel fracture #E and dentin fracture #F • No excessive mobility, no luxation • Occlusion is normal • Charlie is cooperative , but impatient and wiggly
Charlie’s Clinical Appearance • What radiographs would you order for Charlie? • Periapical (pedo occlusal)
Case #3 “Charlie” • What is your plan for treatment and followup care for Charlie? • Smooth #E • GI “Bandaid “ #F or composite if cooperation allows • Periodic clinical and radiographic followup
Case #4 “Davonne” • Davonne is a 12 year old boy with a non-contributory Health History • He and his parents are at your office for comprehensive care. • The chief complaint is “discolored lower front teeth.”
Davonne • What most likely caused this discoloration? • History of primary tooth trauma/intrusion • What are treatment options? • No treatment • Cosmetic bonding