Download
1 / 9
90 likes | 105 Views
Learn about the risks associated with undue insulin/SU therapy in major clinical trials such as VADT, ACCORD, and ADVANCE. Understand the consequences of hypoglycemia and the increased cardiovascular risks linked to certain diabetes treatments.

E N D
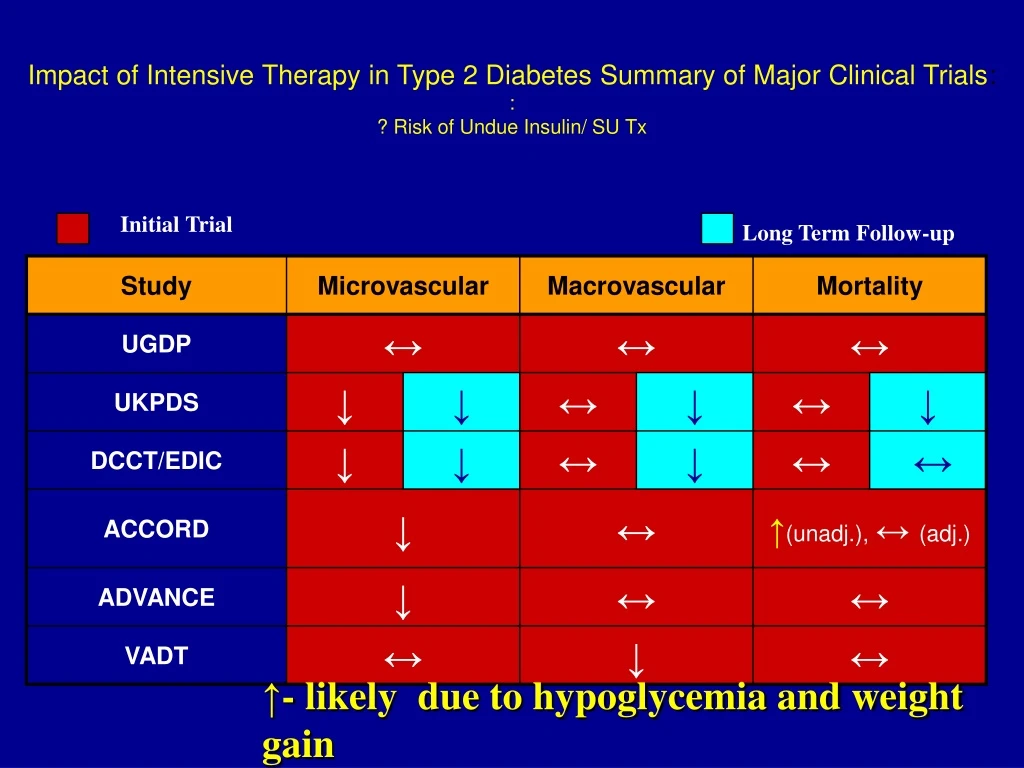
Impact of Intensive Therapy in Type 2 Diabetes Summary of Major Clinical Trials: :? Risk of Undue Insulin/ SU Tx Initial Trial Long Term Follow-up ↑- likely due to hypoglycemia and weight gain
Consequences of Hypoglycemia • Prolonged QT- intervals- Diabetologia 52:42,2009 • Can be of pronged duration IJCP Sup 129, 7/02 • Greater with higher catecholamine levels Europace 10,860 • Associated with Angina Diabetes Care 26, 1485, 2003 / Ischemic EKG changes Porcellati, ADA2010 • Associated with Arrhythmias • Associated with Sudden Death Endocrine Practice 16,¾ 2010 • Increased Variabilty- increases inflammation, ICU mortality Hirsch ADA2010
CV Risk of SU and Insulin So benefit of both SU/Insulin in research studies –UKPDS, DCCT/EDIC But adverse risk in ‘real world’ use- would not pass current FDAguidelines for CV risk with a new agent Pharmacoepidemiology and Drug Safety. 2008;(17):753-759.
Complications CAN Be Reduced; MUST Avoid Hypoglycemia, Weight Gain • DCCT/EDIC and UKPDS- decreased Micro, Macrovascular disease 2. Confusion with VADT, ADVANCE, ACCORD Trials a. Older, longer duration DM, one third with CV disease b. Decreased micro, no benefit CV reduction, ACCORD increased Mortality c. we believe because undue hypoglycemia, weight gain 3. ADA says adjust HgA1c goal Higher if Older, longer duration DM, CV disease 4. I DISAGREE 5. We have 8 classes of drugs that have no undue risk hypoglycemia, weight gain a. so I’m Older, longer duration DM, CV disease -on 3 meds with no undue risk hypoglycemia, weight gain b. my HgA1c 5.4 !!- c. so I still aim for lowest without no undue risk hypoglycemia, weight gain
Philosophy for Reduced Insulin Need in T2DM 1. No Perfect Insulin Exogenous insulin not put in portal system; no fine-tuning a la Beta Cell 2. Leads to Hyperinsulinism- leads to Insulin Resistance (suppresses dopamine in ‘biologic clock’ of hypothalamus)– leads to Increased Weight, Hypoglycemia Risk 3. So Goal of all Insulin Therapy- Least Hypoglycemia, Least Weight Gain 4. Old Logic- use Early Insulin to reduce Glucotoxicity, Lipotoxicity but GLP-1 RAs and SGLT-2 Inh. do that first day!!, with no weight gain, no hypoglycemia 5. Therefore no need for Early Insulin- use 3-4 Non-Insulin therapy before go to Basal Insulin; if start Basal Insulin ,keep Non-Insulin Therapies and 95% of T2DM won’t need Bolus Insulin (by avoiding bolus insulin reduce hypoglycemic risk 85%)