Download

1 / 55
550 likes | 785 Views
APS in Lebanon. Imad Uthman , MD, MPH Professor of Clinical Medicine Head, Division of Rheumatology American University of Beirut Medical Center Beirut, Lebanon.

E N D
APS in Lebanon. ImadUthman, MD, MPH Professor of Clinical Medicine Head, Division of Rheumatology American University of Beirut Medical Center Beirut, Lebanon
Study Of The Clinical And Serological Characteristics And Long-term Evolution of APS PatientsAt The American University of Beirut Medical Center (AUBMC).
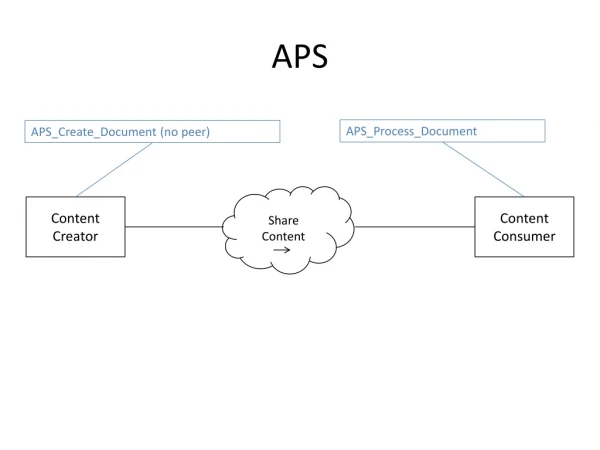
The Lebanese APS Study Group. • Purpose: • To evaluate prospectively the clinical manifestations and the long-term evolution of the APS patients seen at AUBMC and, in the future, expand this to other centers in the country.
The Lebanese APS Study Group. • Methods: • All patients included have fulfilled at least one clinical criterion and one laboratory criterion. • A standardized questionnaire was used to collect demographic data, risk factors for thrombosis, coexisting autoimmune disorders, and specific morbidities due to APS, and data was stored into a registry.
The Lebanese APS Study Group. • Results: • 200 patients logged into the registry so far. • Cases were identified from the lab records (positive ACA and/or LAC tests)
Demographic Cervera R, et al on behalf of the "Euro-Phospholipid Project Group”: Antiphospholipid syndrome: Clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients.Arthritis Rheum 2002; 46: 1019-1027
Underlying Conditions *Cervera R, et al : Arthritis Rheum 2002; 46: 1019-1027
THE LEBANESE APS STUDY GROUP • Results: • In decreasing frequency, the most common complications were: • DVT • Obstetric problems • Stroke • TIA • Seizures • Migraines • Splenic infarcts
THE LEBANESE APS STUDY GROUP • Conclusion: • DVT and strokes are the most common non-obstetric complications of APS in Lebanon. • Many patients suffer from more than one complication, such as DVT or ischemic stroke.
Case Presentation • Mrs. HM 61 year old female presented to ER on March 8, 09 with acute onset of dysarthria and left cheek numbness. • One month before she had recurrent episodes of vertigo and unsteadiness, was told she had ear problems.
Background Hypothyroid and dyslipidemic. Smoker Married 3 children No Hx of abortion, fetal loss, or Preclampsia Hx of premature delivery twice (at 32,30wks) No Hx of DVT.
Physical Exam • BP: 200/100. • Dysarthria. • Right ptosis. • Cerebellar signs: Normal • Gait: Normal • Sensory Exam: Normal
MRI Brain: 9 March 09 Impression: Multiple acute lacunar infarcts in watershed distribution in both centrum semi-ovale as well as in the left precentral gyrus. Subacute infarct in the left occipital area.
Assessment • Neurology: R/O Vasculitis • Rheumatology: R/O APS
Laboratory Evaluation • Lupus anticoagulant:Positive • ACA IgG:96.4 GPLu/mL • ACA IgM: <7 MPLu/mL • Anti ß2-Glycoprotein I IgG:>200 U/ml • Anti ß2-Glycoprotein I IgM: <2 U/ml
Laboratory Evaluation • ANA: Negative • Anti ds-DNA: Negative • C-ANCA: Negative
Course in Hospital Started on Heparin, Plavix. Next day ( March 10) marked improvement in speech
Course in Hospital • March 11: • Worsening dysarthria. • PTT was in the therapeutic range. • Started on Prednisone 1mg/kg by the neurology team (for suspicion of CNS vasculitis).
Course in Hospital • March 14 PM: • Worsening of numbness and weakness in the right upper extremity + had tongue numbness • INR 2.6 • BP: 175/110 • Solu-Medrol 250 mg IV given • Restarted on IV Heparin
Course in Hospital • 15 March Evening: • Acute right sided weakness 0/5 motor power Rt side + Aphasia.
MRI Brain: 15 March 09 • Impression: • Acute infarcts in the left parietal and frontal lobes and in the watershed territories bilaterally more so on the left. • Small focus of hemorrhage in the left parietal lobe.
Course in Hospital • 16 March: • 12 PM: Unconscious, seizure like activity. • Acute respiratory distress: mechanical ventilation. • Physical Exam: • Pupils mid sized dilated • Absent corneal reflex • Absent Oculocephalic reflex • Decerebrate posturing • Bilateral positive Babinski
CT Brain: 16 March 09 • Impression: • Hemorrhagic transformation in the left frontal lobe infarct with significant surrounding edema, mass effect, trans-tentorial and uncal herniations with brain stem infarct.
Course in Hospital • 17 March (one week after her initial presentation): • Declared brain dead, family decided to stop mechanical ventilation.
Nightmare on Bliss Street The Autopsy
Brain Gross Pathology • Soft, edematous • Lt Sub-falcial herniation • Uncal herniation and necrosis.
Terminal Massive ICH • Recent large intracerebral hemorrhage, left frontal and parietal lobes.
Fibrin thrombi within a vessel • Free-floating small fibrin thrombi within rare arterioles and venules in cortex, leptomeninges, and white matter hemorrhage.