Download
1 / 26
260 likes | 348 Views
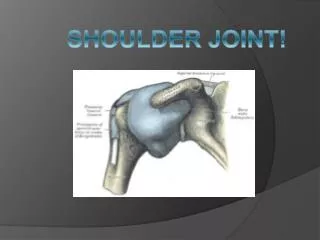
PTA 106 Fall 2008 Shoulder Joint. Candace Rio Alicia. Shoulder Joint. AC ( acromialclavicular ) ligament : extends from the acromium to the clavicle Coracoclavicular ligament : divided into the conoid and trapezoid ligaments

E N D
PTA 106 Fall 2008Shoulder Joint Candace Rio Alicia
Shoulder Joint • AC (acromialclavicular) ligament: extends from the acromium to the clavicle • Coracoclavicular ligament: divided into the conoid and trapezoid ligaments - conoid: apex attaches to the root of the conoid process, base attaches to the inferior surface of the conoid tubercle of the clavicle - trapezoid: nearly horizontal, attaches to superior surface of coracoid process, lateral and posterior to trapezoid line on the inferior surface of the clavicle • Glenohumeral ligaments: part of the fibrous layer of the capsule - coracohumeral: base of the coracoid process to anterior of greater tubercle - transverse humeral: broad fibrous band from greater to lesser tubercle, converts the intertuberclar groove into a canal for the tendon of the long head of the biceps brachii and its synovial sheath • Glenohumeral joint: ball and socket joint, more freedom than any other joint, movement around three axis, allows flexion-extension, abduction-adduction, medial and lateral rotation of the humerous, and circumduction
Cartilage Articular cartilage: caps the surfaces of articulating bones to provide a smooth, low-friction gliding action allowing for free movement Cartilage: avascular and is nourished by diffusion
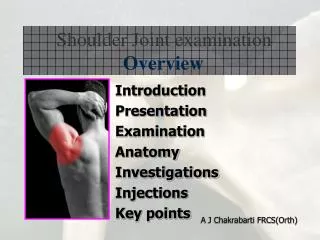
Labrum • Glenoid labrum: ring like, fibrocartilaginous material that adds some depth to the glenoid cavity • Injuries: Baseball players are prone to glenoid labrum tears due to the biceps tendon pulling sharply on the top part of the labrum, golfers who allow their clubs to hit the ground during a swing are also at risk.
Bursae Subacromial (subdeltoid)bursa: facilitates movement of the supraspinatus tendon Subscapular bursa: communicates with the cavity of the glenohumeral joint through an opening in the fibrous layer of the joint capsule
Bursae Continued Subcoracoid Bursa
Articular Capsules • Articular capsule: fiborous capsule lined with a synovial membrane, two articulating bones are joined by the capsule, the outer layer of the capsule is the fibrous layer and the inner layer is the synovial membrane, the joint cavity created, holds the synovial fluid, these synovial joints are functionally the most important and common joints throughout the body • Fibrous layer: surrounds the glenohumeral joint, attaches medially to the margin of glenohmeral cavity and laterally to the anatomical neck of the humerous, superiorly- encloses the proximal attachment of the long head of the biceps brachiito the supraglenoid tubercle of the scapula • Synovial membrane: lining of the interior surface of the fibrous capsule, it reflects onto glenoid labrum and the articular margin of the head of the humerous, forms a tubular sheath for the biceps brachii(longhead), anteriorly- allows for communication between the subscapular bursa and the synovial cavity
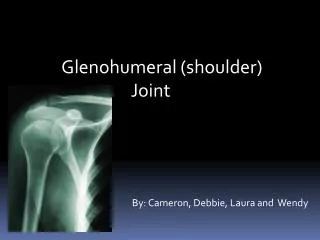
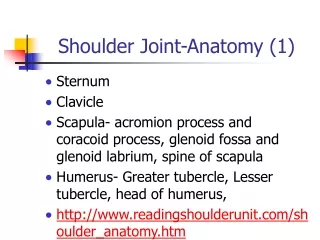
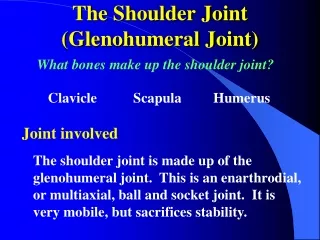
Shoulder Joint Bones Primary Functions Support Protection Assist in Movement Blood Cell Production Storage of Minerals Storage of Chemical Energy • Humerus • Scapula • Clavicle
Scapula Features Acromion Process Borders Superior Vertebral (medial) Axillary (lateral) Angles Superior Inferior Fossae Sub scapular Supraspinatous Infraspinatous Spine GleniodFossa (cavity)
Clavicle • Conoid Tubercle • Acromial End • Articulates with the Acromian Process of the Scapula
Surface Anatomy Anterior Axillary Fold Clavicle Acromial Part of Deltoid Claviclular part of Deltoid Clavipectoral Triangle Clavicular Head of Pec Major Manubrium Sternocostal Head of Pec Major
Surface Anatomy • Posterior Axillary Fold • Spinal Part of Deltoid • Triangle of Auscultation • Borders • Trapezius • Rhomboid Major • LatissimusDorsi • Medial Margin of Scapula
Surface Anatomy • Ascending Part of Trapezius • Middle part of Trapezius • Descending Part of Trapezius
Muscles(origins, insertions, innervations and vascular supplies) • Upper Trapezius • :O Occipital bone, nuchial ligament • I: Outer third of clavical, acromion process • Middle Trapezius • O: Spinous Process of C7-T3 • I: Scapular Spine • Lower Trapezius • O:Spinous processes of Middle and Lower Thoracic • I: Base of Scapular Spine • Innervation: Spinal Accessory • Vascular: Transverse Cervical Artery
Levator Scapulae • O:Transverse of C1-C4 • I: Vertebral border of scapula • Innervation: CN 3&4 • Vascular: Dorsal Scapular Artery • Pectoralis Minor • O: Ant. Surface of 3-5 Ribs • I: Corocoid process of scapula • Innervation: medial pectoral nerve • Vascular: axillary nerve • Serratus Anterior • O: Lateral surface of ribs 1-8 • I: Vertebral border of scapula • Innervation: long thoracic nerve • Vascular: lateral thoracic artery
Rhomboid Major • O:spinous process of T2-T5 • I: Vertebral border of scapula • Rhomboid Minor • O: spinous process of C7-T1 • I: Vertebral border of scapula • Innervation: dorsal scapular nerve • Vascular: Dorsal Scapular Artery
Anterior Deltoid • O:Lateral third of clavicle • Middle Deltoid • O: Acromion Process • Posterior Deltoid • O: Spine of Scapula • I: Deltoid Tuberosity • Innervation:. Axillary Nerve • Vascular: Posterior circumflex artery
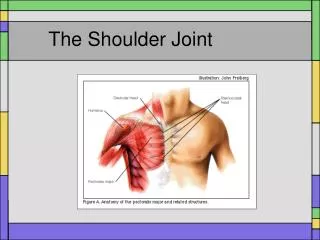
Pectoralis Major • O: Medial third of clavicle, sternum, cartilage of 1-6 ribs • I: Lateral lip of bicipital groove. • Innervation: lateral and medial pectoral nerve • Vascular: lateral thoracic artery • Teres Major • O: Axillary border of scapula • I: Crest below lesser tubercle of humerus • Innervation: subscapular nerve • Vascular: circumflex scapular artery
LatissimusDorsi • O: Spinous process of T7-L5, Posterior surface of sacrum, Iliac Crest, lower three ribs. • I: Medial lip of bicipital groove • Innervation: thoracodorsal nerve • Vascular: Deep scapular artery • Coracobrachialis • O: corocoid process • I: Medial aspect of humerus • Innervation: C6&C7 nerves • Vascular: Brachial Artery
Rotator Cuff • Teres Minor • O: Axillary border of scapula • I: Greater tubercle of humerus • Innervation: axillary nerve • Vascula: circumflex scapular artery • Supraspinatus • O: Supraspinatusfossa of scapula • I: Greater Tubercle of humerus • Infraspinatus • O: Infraspinatusfossa of scapula • I: Greater Tubercle of humerus • Innervation: Suprascapular nerve • Vascular: Suprascapular artery • Subscapularis • O: Subscapularfossa of scapula • I: Lesser Tubercle of humerus • Innervation: Subscapular nerve • Vascular: Subscapular artery
Rotator Cuff Injury • What is it? Rotator cuff injury can be as simple as an inflammation of the muscle, (tendonitis) to a complete or partial tear of the muscle that may lead to surgery to correct. • Causes Chronic Tear: sports, jobs that require excessive overhead activity i.e. pitchers, painters (occurs more often in dominant arm) Acute Tear: sudden powerful raising of arm against resistance (often in attempt to cushion a fall) significant amount of force needed. Tendinitis: degeneration of muscle with age. Repetitive trauma to muscle by everyday movement of shoulder. (May lead to chronic tear.)
Testing for Rotator Cuff Injury Inpingement Injection Test: Doctor raises arm of pt forward to see if it causes pain. If it does lodocaine (a numbing agent) is injected into muscle and test is preformed again. If there is no pain pt is said to have tendinitis or a small tear in the rotator cuff. Drop Arm Test: Doctor raises arm at a 90 degree angle and has pt hold it in that position. Dr. applies slight pressure to forarm and wrist that may cause pt to drop wrist suddenly. This is a sign of a significant tear. Treatment • rest shoulder • Ice first 2 days then heat • Ibprofen-naproxen • Possible steriod injection • Sling • Possible surgery • PROM excercises
Follow up: work with PT. Orthopedic surgeon can evaluate further need for surgery. Prevention: avoid landing on shoulder in sports or falls… Easier said than done. Seek early medical attention if shoulder pain develops because of over use.
AND IF YOU DON’T KNOW NOW YOU KNOW