Download
1 / 1
10 likes | 113 Views
How can we ascribe consciousness: Finding the Voice of Vegetative State Patients. Aghaki -Allen L, Berger R, McKenna O, Sainsbury T and Vinsland E. . Introduction.

E N D
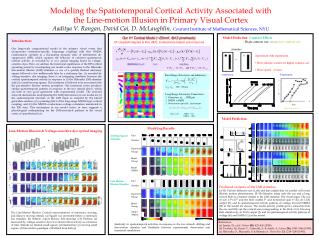
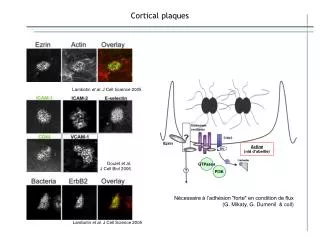
How can we ascribe consciousness: Finding the Voice of Vegetative State Patients Aghaki-Allen L, Berger R, McKenna O, Sainsbury T and Vinsland E. Introduction Severe trauma or hypoxia can lead to a persistent vegetative state (PVS) in which patients that have emerged from a coma appear to be awake. They still retain reflex brain functions such as a sleep-wake cycle, random eye movements and grimaces at pain. Unlike locked-in patients, which may outwardly appear similar, they are unable to communicate through behaviour. This has led to many believing they are unconscious. However, recent technological advances have improved our understanding, indicating the brain areas needed for cognition, perception , memory and intention, may be undamaged in some cases. This begs the question: are they conscious? 1. History • First coined by Jennet and Plum (1972)based on the definition of vegetative: ‘An organic body capable of growth and development but devoid of sensation and thought.’ • The phrases used are indicative of the thought at the time: ‘a mindless state’, wakefulness without awareness’, ‘eyes open unconsciousness’ and ‘absence of function in the cerebral cortex’ (Jennett and Plum 1972; Cranford 1988). • They judged a lack of function to mean a lack of consciousness and made these assessments on behavioural observations alone. • This lead to, in some cases, people considering their treatment futile (Schneiderman et al 1990). Fig1: The original classification of the vegetative state as ‘high arousal, low consciousness’ 2. Preservation of Cortical Activity 3. Wilful Modulation of Brain Activity • Brain imaging studies show some islandsof cortical activity can be preserved. PET scans in one patient showed when presented with a familiar face, the fusiform face area was active. However it could just be automatic processing without conciousness. • Ambiguous words activated areasknown in semantic processing (superiorand middle temporal gyri.) – something not seen in healthy controlswhen they areanaesthetised, suggesting somelanguage comprehension • Using real time fMRI,a patient showed willful intention. She was • played a pre-recorded instruction • asking her to imagine either • playing tennis or walking around • her house for a period of time • (30sec) until told to relax. • Using the same motor and spatial imagery task, a study showed that 5/23 patients diagnosed to be in a vegetative state could wilfully modulate their brain activity. sign of awareness and volition = “minimally conscious” diagnosis based on behaviour – did not reflectawareness and cognitive functioning • One VS patient was able to answer yes-or-no autobiographical questions using motor imagery as “yes” and spatial imagery as “no”. • 100% correct answers from the patient patient could apply imagery technique for communication used to minimise misdiagnosis ask patients if they are in pain • Another study asked the patient to move his left and right hands • EEG showed modulation of sensorimotor area patient attempted to move, but unable to execute it can be used for application of prosthetics. Fig 2: The metabolic activity seen in vegetative states is typically 60% less than healthy controls, but still significantly more than in brain dead patients Fig 4: fMRI communication scan showing same areas of activation in control and patient upon using motor and spatial imagery for yes-and-no questions. Fig 3: The BOLD signal in the PVS patient is very similar to that seen in healthy controls when completing the same imagery tasks. 4. Future Directions 5. Ethics • “Outwardly unresponsive” • Change the clinical criteria for PVS and improve quality of life. • Patients can say if they are in pain, specify entertainment and communicate with family. • On the basis that patients are not conscious, current UK laws allows for the removal of assisted nutrition and hydration (ANH) leading to death. • But in the light of this research; is it justifiable to take life, knowing some patients are conscious? And are they able to make the decision themselves? • Does it beg the question; “DO YOU WANT TO DIE?” • For patients that fail these tests, it does not necessarily mean they are unconscious, other factors could inhibit them from responding, so what decisions are to be made about their welfare? • Technological advances in neuroimaging and EEG-based brain-computer interfaces offer possibilities for better diagnostic, prognostic, and therapeutic management • Makes distinction between ‘minimally conscious’ and vegetative state patients possible reduce the errors of diagnosis (40%) • fMRI and EEG recordings could provide a possible mean for communication • Vegetative state patients showed signs of attentive awareness and ability to follow command • Possibility to bedside communication • Clinical importance • Monkeys able to use ‘brain power’ to move prosthetic arm • Use of brain activity for more than just communication? Fig5: EEG recorded brain activity in VGS patients to words which they were told to pay attention to in comparison to ‘distracting’ words. Conclusion • PVS patients were originally thought to lack consciousness. • Advancement in technology has indicated that regions of cortical activity can be preserved. • Some PVS patients have demonstrated clear volition – showing consciousness. • Challenge: translating this research into clinics to provide correct and cost effective diagnosis and communication. • Prospect: Jean-Dominique Bauby, the famous writer and editor of French magazine’ Elle’, who while suffering from locked-in syndrome wrote a book through the blinking of his eye. Fig6: Owen, one of the pioneers in studying PVS, wearing an EEG cap Beaumont J.G, .Kenealy P.M. (2005) Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil.15(3-4):184-9. Chennu, S., Finoia, P., Kamau, E., Monti, M., Allanson, J., Pickard, J., Owen, A. and Bekinschtein, T. 2013. Dissociable endogenous and exogenous attention in disorders of consciousness. NeuroImage: Clinical, (3): 450-461. Cologan V., Schabus M., Ledoux D., Moonen G., Maquet P. & Laureys S. (2010). Sleep in disorders of consciousness. Sleep Med Rev. 14(2): 97-105. Constable C. (2012). Withdrawal of artificial nutrition and hydration for patients in a permanent vegetative state: changing tack. Bioethics. 26(3): 157-63. Cranford R. (1988). The Persistent Vegetative State: The Medical Reality (Getting the Facts Straight). The Hastings Centre. 18: 27-32. Cruse D., Chennu S., Fernández-Espejo D., Payne W.L.,Young G.B. & Owen A.M. (2012). Detecting Awareness in the Vegetative State: Electroencephalographic Evidence for Attempted Movements to Command. PLoS One. 7(11): e49933. Cyranoski D. (2012) Neuroscience: The Mind reader. Nature. 486: 178–180. Golan O.G., Marcus E.L. (2012). Should we provide life-sustaining treatments to patients with permanent loss of cognitive capacities? Rambam Maimonides Med J. 3(3). Jennett B. & Plum F. (1972). Persistent vegetative state after brain damage: a syndrome in search of a name. Lancet. 1: 734-737. Menon D.K., Owen A.M, Williams E.J., Minhas P.S., Allen C.M.C., Boniface S.J., Pickard J. D., (1998) Cortical processing in persistent vegetative state. Lancet. 352: 200. Monti M., Laureys S. & Owen, A. (2010). The vegetative state. Bmj. 341:c3765. Monti M., Vanhaudenhuyse A., Coleman M., Boly M., Pickard J., Tshib A.L., Owen, A. and Laureys, S. 2010. Willful modulation of brain activity in disorders of consciousness. New England Journal of Medicine. 362 (7): 579-589. Owen A.M., Coleman M.R., Boly M., Davis M.H., Laureys S., Pickard J. D. (2006) Detecting Awareness in the Vegetative State. Science. 313: 1402 Schneiderman L., Jecker N. & Jonsen A. (1990). Medical Futility: Its Meaning and Ethical Implications. Ann Intern Med. 112, 949-954. Shea N., & Bayne T. (2010). ‘The vegetative state and the science of consciousness.’ Brit. J. Phil. Sci. 61: 459– 484. Velliste M., Perel S., Spalding M., Whitford A. & Schwartz A. (2008). Cortical control of a prosthetic arm for self-feeding. Nature. 453 (7198): 1098--1101. End of life care: Clinically assisted nutrition and hydration. Based on NICE guidelines Retrievedfrom:http://www.gmcuk.org/guidance/ethical_guidance/end_of_life_clinically_assisted_nutrition_and_hydration.asp Date accessed:10/12/2013, 23:01.