Download
1 / 18
570 likes | 2.44k Views
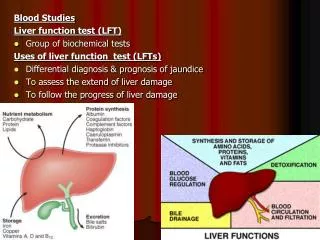
Liver Function Tests (LFTs). Major Metabolic F unctions of the Liver. Synthetic functions Proteins: plasma proteins albumin , globulins, coagulation factors…etc ) Lipids: cholesterol, triglycerides, fatty acids, phospholipids & lipoproteins (VLDL)

E N D
Major Metabolic Functions of the Liver • Synthetic functions • Proteins: plasma proteins albumin, globulins, coagulation factors…etc ) • Lipids: cholesterol, triglycerides, fatty acids, phospholipids & lipoproteins (VLDL) • Carbohydrates: glycogen synthesis & gluconeogenesis • Detoxification & excretion functions - Detoxication of ammonia to urea (urea cycle) - Billirubin conjugation & excretion into bile - Excretion of cholesterol into bile - Drug detoxication & excretion into bile • Storage Function - Storage of fat soluble vitamins (vitamins A, D, E & K) • Storage of vitamin B12 • Production of bile salts - Help digestion of lipids
Liver function tests (LFTs) Overview LFTs are blood tests used to help to diagnose & monitor disease or damage of the liver The tests measure the levels of certain enzymes & proteins in blood Some of these tests measure how well the liver is performing its normal functions of producing protein & clearing billirubin. Other liver function tests measure enzymes that liver cells release in response to damage or disease. However, 1- Conditions other than liver disease or damage can lead to abnormal liver function test results 2- Test results can be normal in people who have liver disease or damage
Liver function tests can be used to: 1- Check certain enzymes & proteins levels in blood that if are higher or lower than normal can indicate liver problems (diagnosis) 2- Screen for liver infections, such as hepatitis 3- Monitor the progression of a liver disease, such as viral or alcoholic hepatitis & determine how well a treatment is working (prognosis) 3- Measure the severity of a liver disease especially liver cirrhosis 4- Monitor possible side effects of medications on liver 3-
Routine Liver Function Tests (LFTs) 1- Serum Albumin 2- Blood Liver Enzymes: Alanine amino transferase (ALT) Aspartate amino transferase (AST) Gamma glutamyl transferase (GGT) Alkaline phosphatase (ALP) 3- Blood Billirubin (total, direct & indirect) 4- Blood Coagulation Factors (prothrombin & others) Prothrombin Time (PT) Others: Markers of liver fibrosis
Serum Albumin • Albumin is present in higher concentrations than other plasma proteins ( ~ 40 g/L in normal adults). • Albumin is synthesized in the liver & has a half-life of 20 days. • Very small amounts of albumin cross the glomerular capillary wall. Accordingly, no more than traces of albumin may normally appear in urine that can not be detected by ordinary laboratory means. • Albuminuria: In this case, albumin can be detected in urine by ordinary laboratory means due to physiological or pathological conditions.
Serum Albumin cont. Causes of hypoalbuminemia Artfuctual : Diluted sample Physiological : Pregnancy - Recumbence Decreased amino acids : Reduced essential amino acids in diet & reduced synthesis of nonessential amino acids Malnutrition Malabsorption. Increased catabolism : Surgery Trauma Infections Defective synthesis in liver: Chronic liver diseases Increased loss : From the kidney: Nephrotic syndrome From GIT: Protein loosing entropathies
Blood Aminotransferases (ALT & AST) • Aminotransferases (ALT & AST) are normally intracellular enzymes • Plasma contains low levels of aminotransferases representing release of cellular contents during normal cell turnover • Elevated blood levels of aminotransferases indicate damage to cells rich in these enzymes (as disease to tissue or physical trauma ) • Blood AST & ALT are of particular diagnostic value
Causes of elevated levels of blood ALT & AST • 1- Viral, toxic or alcholichepatitis • ALT & AST are elevated even before appearance of clinical signs (jaundice) & symptoms. • Markedincrease in ALT & AST (Up to 20 - 50 - may reach up to 100 folds). • Peak values between 7 – 12 days of onset of the disease • In viral hepatitis, ALT is muchelevated than AST • 2- Cirrhosis (chronic liver diseases) • ALT & AST are increased to levels depending on the status of the process • (Moderateincrease (up to 4 – 5 folds) • In chronic cases, AST is muchelevated than ALT. • 3- Obstructive jaundice: • ALT & AST are increased up to 3 folds (moderate increase) • 4- After alcoholic or drug intake(transient slight to moderate increase).
Alanine amino transferase (ALT) • ALT is moreliver specificthan AST. • ALTrarely increases in lesions other than the liver parenchymal • ALTelevations persist longerthan do AST. • Aspartate transaminase (AST) • Blood levels of ASTare increased with many diseases of various organs: • 1- Liver diseases • 2- Myocardial infarction (MI) • However, ALT may be also increased if liver congestion occurs secondary to congestive heart failure • 3 - Progressive skeletal muscular dystrophy • 4- Crush injury • 5- Hemolytic diseases • 6- Artifact: in hemolysed samples or if serum separation is delayed
Gamma glutamyl transferase (GGT) • GGTpresent in blood originates primarily from hepatobillarysystem • Causes of increased blood GGT: • 1- Induction of GGT synthesis by these cells occurs without cell damage • by alcohol or drugsas anticonvulsants , phenobarbitone & phenytoin • 2- Biliary obstruction: • GGT is markedly increasedwith obstructive jaundice (5 – 30 folds) • Increase earlier (more sensitive) than ALP • Persists longerthan ALP • 3-Viral, toxic & alcoholic hepatitis : • Increase is only 2 – 5 folds (less sensitive than ALT & AST) • 4-Primary and secondary liver tumors: • GGT is elevated earlier than other enzymes in liver neoplasm. • Secondaries of other organ tumors in the liver can be early detected by • elevated GGT. (arouse suspicious that the diseases is metastatic to liver)
Alkaline Phosphatase (ALP) • Alkaline phosphatases (ALP) are group of enzymes that hydrolyze organic phosphates at high pH (9 – 10.5) • Main Sources of ALP: • 1- Cells of hepatobiliary tract (hepatocytes adjacent to the biliary canalculi) • Activity in the liver is localized on those parts of the cell membrane of the • parenchymal cell adjoining the biliary canalculi • 2- Osteoblasts of bone : • he metabolic function of ALP is probably important for bone calcification. • Other Sources: Intestine and placenta & renal tubules
Alkaline Phosphatase (ALP) cont. • Clinical significance of increased serum ALP activities: • 1-Physiological increase of ALP: • During periods of active bone growth in infancyand at puberty • Preterm infants total ALP is increased to 5 times the upper reference limit of adults due to bone isoenzymes. • In children under 3 years, total ALP activity is increased up to 2.5 times the upper limit • Increased twice, during the second andthird trimesters of pregnancy (placental ALP).
Alkaline Phosphatase (ALP) cont. • 2- Pathological increase of ALP: • A-Bone causes (due to increased osteoblastic activity): • Tumors (osteogenic) • Paget`s Disease of bone • Marked increase , may be 10 – 25folds) • due to osteoblastic cells action trying to rebuild bone that is resorped by activity of osteoclasts • Primary osteogenic tumors • Secondary malignant deposits in boneif causing osteoblastosise.g. cancer prostate causing deposits in bones (osteoblastic tumor) • Rickets & osteomalacia (vitamin D deficiency) • Primary & secondary hyperparathyroidism (increased PTH) • Healing of bone fractures
Alkaline Phosphatase (ALP) cont. • B-Hepatobiliraytract • liver diseases with involvement of biliary tract • 1- Obstructive jaundice(intrahepatic or extrahepatic) • Extrahepatic cholestiasis : (Markedincrease, up to 10 – 12 folds) • Due to obstruction of to the flow of bile through the biliary tract by: • Stones, inflammation of biliary tract or pressure from outside by cancer head of pancreas. • Intrahepatic cholestiasis: (Moderateincrease , ~ 3 -5 folds) • Bile secretion from the hepatocytes into the canalculi is impaired by: • Drugs (chlorpromazine), alcohol, inflammation of the biliary tract (cholangitis). • 2- Viral, toxic & alcoholic hepatitis • Mild to moderate increase, less than 3 folds (ALP may be may be normal)
If ALP is elevated due to a bone disease • In this case, GGTis (or may be) normal • i.e. GGTis used to ascertain whether increased ALPis due to boneor hepatobiliary disease
Coagulation factors • The liver makes many of the proteins (prothrombin & other clotting factors) needed to make blood clot • In certain liver disorders the liver cannot make enough of these proteins and so blood does not clot so well. Therefore, blood clotting tests may be used as a marker of the severity of certain liver disorders • In liver disease, the synthesis of prothrombin & other clotting factors is diminished, prolonged prothrombin Time (PT) • This may be one of the earliest abnormalities seen in hepatocellular damage, since prothrombin has a short half-life (~ 6 hours)
Makers of Liver Fibrosis • Procollagen type III terminal peptide • Hyaluronic acid (hyaluronin)