Download
1 / 25
250 likes | 286 Views
Understand bariatric procedures, surgery requirements, post-op nutrition therapy, lifestyle changes, and ethical issues. Learn about obesity statistics, common surgeries like Roux-en-Y and Laparoscopic Band, and the importance of supplementation.

E N D
BariatricSurgeryEmily SchwichtenbergConcordia CollegeMoorhead, Minnesota
Objectives • To explain different bariatric procedures • Discuss requirements for surgery • Explain post-op medical nutrition therapy • Discuss proper and important lifestyle changes • Discuss ethical issues
Obesity as an Epidemic Statistics • 66.3% of United States adults are overweight • 32.2% are obese with a BMI >30 kg/m² • 4.8% are morbidly obese with a BMI >40 kg/m² • From 1986-2000 BMI >30 kg/m² doubled in the United States • BMI of >40 kg/m² quadrupled • BMI of >50 kg/m² increased fivefold Schernthaner, G., & Morton J.M. (2008). Bariatric surgery in patients with morbid obesity and type 2 diabetes. Diabetes Journal, 31, 297-302.
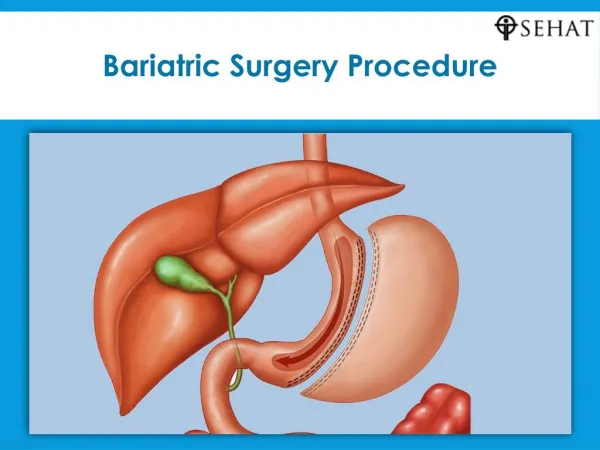
Roux-en-Y • Most common procedure • Upper portion of stomach is stapled and separated • Small intestine is cut and attached to the small pouch • Small intestine is reconnected with rest of intestine • New stomach is about the size of your thumb Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Laparoscopic-Band • A ring or a band is placed around the upper portion of the stomach • Small opening at the bottom of the pouch to allow food to pass slowly into the rest of the stomach • Port underneath abdomen that controls the tension on the band Nelms, M, Sucher, K., Long, S. (2007). Nutrition Therapy and Pathophysiology. Belmont, CA: Thomson Higher Education.
Biliopancreatic Diversion/ Duodenal Switch • Not used due to malabsorption issues • Lower portion of stomach is removed • Directly connected to the lower part of the small intestine • Duodenum is completely bypassed • High mortality rate and increased long term conditions U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, & National Institutes of Health. (March, 2008). Bariatric surgery for severe obesity. Retrieved September 29, 2008, from http://win.niddk.nih.gov/publications/gastric.htm#bbypass
Vertical Banded Gastroplasty • Small vertical pouch surgically created at top of stomach • Line of staples through both walls • Band controls volume of pouch • Prevents stretching • Restricts amount of food patient can eat Nelms, M, Sucher, K., Long, S. (2007). Nutrition Therapy and Pathophysiology. Belmont, CA: Thomson Higher Education.
The Common Procedures Roux-en-Y Laparoscopic Adjustable Band • Invasive but considered the gold standard • Fast weight loss averaging 70-80% with in 2 years • Fast resolution of co-morbidity conditions ( esp. type-II diabetes) • Best for patients with BMI > 50 • Best for patients with severe co-morbidity conditions • Vigorous vitamin and mineral supplementation • New technology- simpler procedure • Slow, yet steady, weight loss averaging 50% from 2-5 years • Slower resolution of co-morbidity conditions • Best for younger patients with BMI <50 • Less vigorous vitamin and mineral supplementation • Faster recovery and return to work Leah Walters, Mari Willie. Pre-surgical bariatric patient class. Unpublished manuscript.
Weight Changes among subjects participating in the Swedish Obese Subjects study over a 10-year period. 627- control subjects 156- laparoscopic adjustable banding subjects 451- vertical banded gastroplasty subjects 34 – Roux-en-Y gastric bypass subjects Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Requirements for Surgery • BMI >40 kg/m² or BMI >30 kg/m² and suffer with co-morbidities • Weigh over twice your ideal body weight • Understanding that surgery is a tool not a cure and the change will come with overall lifestyle change • Most facilities and insurance agencies have other requirements that one must meet before the procedure Schernthaner, G., & Morton J.M. (2008). Bariatric surgery in patients with morbid obesity and type 2 diabetes. Diabetes Journal, 31, 297-302.
Medical Nutrition Therapy: Diet Change • 2-3 weeks post-op clear liquid diet and progress to full liquid diet • 3-4 weeks post-op semisolid or soft foods • 4 ounces at a time • Every 3-4 hours • 4-5 weeks post-op try solid foods one at a time • Must eat slowly at least 20-30 minutes per meal • Must chew until food is a liquid consistency in mouth • Must drink at least 64 ounces of liquid through the day • Do not drink 20 minutes before meal • Do not drink 20 minutes after meal • Do not drink during meal • Vitamin, mineral and protein supplementation Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Supplementation • With the limited diet patients will not get RDA for certain vitamins and minerals • Vitamin B12, Iron, Folate, Calcium, Vitamin D, Vitamin A • Adequate protein intake is crucial for healing post-op • Can be taken in a multi-vitamin or separate daily • Make sure all supplements are chewable • Must have correct dosage in multi-vitamin Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Supplementation: B12 • 300-500µg/d • Sublingual form (under the tongue) • Deficiency seen in 64% of Roux-en-Y patients (Shah et al, 2006). • Important for protection of the nerve cells. Needed for cell synthesis and helps break down some fatty acids and proteins • Deficiency causes anemia, fatigue, degeneration of peripheral nerves Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Iron • Deficiency seen in 52% of Roux-en-Y patients (Shah et al, 2006) • Take with vitamin C to increase absorption • 320 mg daily • Prevents anemia • Iron carries oxygen to cells importantly muscle cells • Deficiency causes anemia Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Folate • Deficiency seen in 34% of Roux-en-Y patients (Shah et al, 2006) • 400-1000 µg/d daily intake • Increased rate of neural defects in children born to Roux-en-Y mothers • Helps with protein synthesis • Deficiency causes anemia, weakness, confusion Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Calcium • Deficiency seen in 10% of surgical patients • Recommended intake 1200-1500 mg/d • Take twice daily 500-600 mg/d due to absorption rate • Deficiency is not always apparent at first because of calcium releasing from the bone • calcium citrate supplement more effective than calcium carbonate • Deficiency is seen as stunted growth in children and osteoporosis in adults Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Vitamin D • Deficiency seen in 51% of patients • Recommended supplementation is 400 IU/d • Recommended to take separate than iron supplement due to absorption • Important for bone health • Deficiency is seen as rickets in children and osteomalacia in adults Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Vitamin A • 10% of Roux-en-Y patients adapt vitamin A deficiencies • It is recommended to have supplementation as needed based on physician monitoring • Deficiency is due to some fat malabsorption • Important for sight and skin health • Deficiencies include: decreased immune function, blindness, night blindness, and some skin conditions Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Protein • Protein is important post-op to help heal the surgical wound • Recommended 65 grams per day • Supplementation should be 200 calories with 15 grams of protein • High Protein Foods • Fish • Lean cuts of beef or pork • Skinless chicken or turkey • Dry beans/legumes • Egg whites • Non-fat or low-fat milk and milk products • Nuts and peanut butter Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Nutrition Care Process • Assessment • Age, weight and height • BMI, and IBW • Nutrient intake • Diagnosis • Co-morbidities • Obesity • Intervention • Weight loss program • Bariatric surgery • Vitamin regimens • Exercise regimens • Monitor • Follow-up appointments • Vitamin regimens • Exercise regimens
Lifestyle Change • Exercise • 30-6o minutes 3-5 days a week • Weight loss changed from 70% baseline to 90% baseline with exercise (Shah et al, 2006). • Strength training 2-3 times per week • Positive attitude • Surround yourself with a positive social support group • Easier to manage stress Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Ethical Issue: Overall Cost • Approximately $30,000-$50,000 for the surgery alone • Can vary depending on health care facility • Approximately $100 monthly for vitamin supplements • Can vary on brand and purchase company • $250-$300 for protein supplements • Dependent on brand Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Ethical Issue: Insurance Coverage • Insurance will cover surgery • Insurance will not cover preventative care • Dietetic counseling before obesity gets out of control • Personal training sessions • Insurance will not cover vitamin supplementation • This is a huge cost post-op • Due to surgery supplementation is crucial
Ethical Issue: Surgical Requirements • The strict requirements may lead patients to gain weight before applying for insurance • Some facilities require weight loss before surgery • Insures seriousness of patient • Provides positive feedback for patient • Learn new lifestyle • If gaining weight to meet BMI requirements patient is not learning the new lifestyle • Find a workout routine that works for them