Download
1 / 22
220 likes | 393 Views
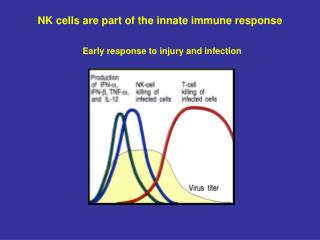
The Innate Immune Response. Chapter 15. The “Good” Immune Response. The immune response’s principal objective is the containment of infectious threats Most of the time, containment requires elimination of the microbe ( sterilizing ) But sometimes it is sequestration of a pathogen

E N D
The Innate Immune Response • Chapter 15
The “Good” Immune Response • The immune response’s principal objective is the containment of infectious threats • Most of the time, containment requires elimination of the microbe (sterilizing) • But sometimes it is sequestration of a pathogen • These objectives are accomplished by a highly coordinated series of events • Many types of cells • Many soluble molecules • It also provides long-term memory
The “Bad” Immune Response • The immune response is inherently dangerous • Its job is to kill infectious agents • Sometimes it kills the body’s own cells in doing so • If sufficient damage is done by the immune response, it can cause the death of the patient • Disease and death caused by the immune response is immunopathology
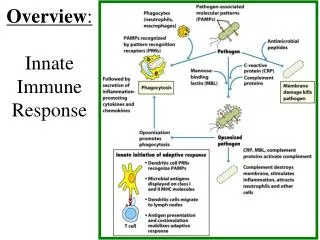
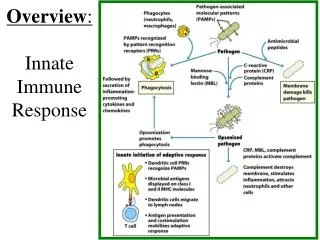
The Phases of the Immune Response • The innate phase • Considered “nonspecific” (a misnomer) because it recognizes common molecules of microbes • Pattern recognition receptors (PRR) are proteins that bind to a broad-spectrum of microbial products • Lipopolysaccharide • Double-stranded RNA • Molecules of the innate phase are ever-present, thus act immediately upon a danger signal
The Phases of the Immune Response • The adaptive phase • Becomes apparent within a few days after infection • Principally mediated by two types of cells • T cells that secrete cytokines (which are proteins) that mediate local immune responses • B cells that secrete high affinity antibodies that noncovalently bind to microbes and their products • Together, these cells control the great majority of infections • It also provide long-term memory to infectious agents, such that disease rarely recurs • It also is responsible for immunopathology
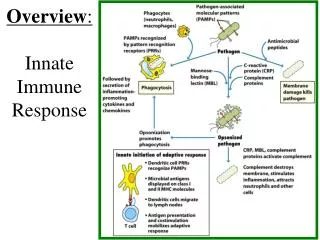
15.1 Overview of Innate Defenses • Portals of entry are those where microbes have an opportunity to access the body • First-line defenses • Skin • Mucosa • PRR, including Toll-like receptors (TLRs) found on phagocytic cells • Complement proteins • Inflammation • Fever
15.2 First-Line Defenses • Physical barriers • The mucosa contain many substances that are toxic to microbes • Defensins are antimicrobial peptides about 30 amino acids in length • Peroxidase is an enzyme that causes oxidation of microbial products • Lysozyme degrades peptidoglycan • The skin possesses the water-tight protein polymer keratin that is resistant to penetration • Normal flora are the bacteria that inhabit the body and protect against other infectious agents • Staph epidermidis outcompetes Staph aureus
15.3 The Cells of the Immune System • All cells of the immune system arise in the bone marrow • Stem cells of various developmental maturity exist in the bone marrow and are precursor cells for immune and blood cells • Hematopoiesis is the process of generating and maintaining immune and blood cells • The process of immune and blood cell formation is mostly unknown and considered the Holy Grail of immunology • Special cytokines, termed colony stimulating factors (CSF) play a prominent role in hematopoiesis, but bone marrow stromal cells are also required
15.3 The Cells of the Immune System • Granulocytes • The granules are toxic substances, such as histamine • Neutrophils are highly phagocytic and produce oxidative substances • Basophils and mast cells contribute to inflammation • Eosinophils are thought to play a role in containing parasitic infections • Mononuclear phagocytes • Circulating monocytes exit the blood vessel into a tissue and differentiate into macrophages • These macrophages play a prominent role in constraining microbes to the infected tissue
15.3 The Cells of the Immune System • Dendritic cells • Extremely rare • Reside in all tissues • Provide a link between the innate response and the adaptive response by stimulating naive T cells • Lymphocytes (Adaptive Response) • T cells • Helper T cells secrete cytokines • Cytotoxic T cells kill other cells that harbor pathogens • B cells secrete antibodies (aka, immunoglobulins) • Natural killer (NK) cells kill infected cells (and cause collateral damage by killing adjacent, uninfected cells)
15.4 Cell Communication • Cytokines are secreted by all cells of the body • There are more than 60 known cytokines in vertebrates • They have a dramatic impact on immune responses • Can be secreted in large amounts • Are not restricted to the tissue • Functional at very low concentrations • They bind to specific cytokine receptors, which results in a physiologic change in the recipient cell • Alterations in gene expression • DNA synthesis
15.4 Cell Communication • Classes of cytokines • Chemokines • Recruit immune cells into infected tissues (”help!”) • Participate in inflammation • Interferons - confer antiviral status upon cells • Interleukins • Largest group • Mediate immune responses • Tumor necrosis factors • Initiate inflammation • Induce programed cell death of infected cells
15.5 Sensor Systems • Vertebrates are under constant microbial threat • Evolution has provided a number of sensing systems capable of recognized these threats • Some complement proteins recognize bacterial cell walls and perforate them • Other complement proteins bind to bacteria and facilitate their phagocytosis • Interferons induce the expression of RNase L, which digests double-stranded RNA
15.6 Phagocytosis • Phagocytic (”to eat”) cells have receptors on their surfaces that bind to bacterial products and complement proteins • They are recruited to sites of infection by chemokines • After engulfment of microbes into a phagosome, the cells are killed by fusion of the phagosome with a lysosome (termed phagolysosome), which contains toxic compounds • Some microbes have evolved mechanisms for evading phagocytosis
15.7 Inflammation • Inflammation is mechanism for containment of microbes in the infected tissue • It is a double-edged sword: • Too little and the microbes can go systemic • Too much and it can lead to cardiovascular shock
15.7 Inflammation • The process • Infected or traumatized tissues secrete chemokines • Circulating leukocytes (white blood cells) exit the blood vessel (diapedesis) by squeezing between capillary endothelial cells • Once in the tissue, the cells secrete inflammatory proteins that augment capillary leakage • The tight junctions between capillary cells loosen • The blood plasma, which is under high pressure relative to the tissue, leaks from the vessel and into the tissue • If the gaps between capillary cells are large enough, red blood cells will also leak into the tissue (hemorrhage)
15.7 Inflammation • Bacterial Endotoxins (e.g., LPS) • Potent inducers of inflammation • Bind directly to macrophages and elicit TNF production • If enough macrophages are stimulated, as in septicemia, then septic shock can occur • In septic shock, so much plasma leaks from the capillaries that the circulatory system collapses • Disseminated intravascular coagulation (DIC) ensues, causing systemic blood clots • The heart cannot continue to pump and the patient dies
15.9 Fever • Fever is caused by the production of interleukin-1 • IL-1, a pyrogen, travels through the blood to the brain, where it acts upon the hypothalamus to increase body temperature • Many bacteria are killed or retarded by high temperatures • Some immune molecules work at higher temperatures • Moderate fever is good for the immune response