Download
1 / 45
450 likes | 639 Views
Chlamydia. Filename: Chlamydia.ppt. Chlamydia. Chlamydia. Obligate intracellular coccoid parasites contain DNA and RNA, and ribosomes lack ATP, biosynthetic pathways cell wall but peptidoglycan absent - use disulfide bonds non motile. Obligate Parasites .

E N D
Chlamydia Filename: Chlamydia.ppt
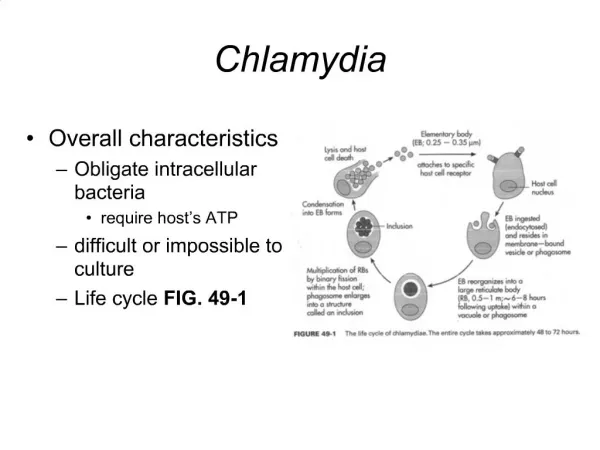
Chlamydia • Obligate intracellular coccoid parasites • contain DNA and RNA, and ribosomes • lack ATP, biosynthetic pathways • cell wall but peptidoglycan absent - • use disulfide bonds • non motile
Obligate Parasites • Obligate intracellular parasites of mammals and birds • not transmitted by arthropods. • incorrectly called the PLT viruses or Bedsonia or basophilic viruses, • Multiply in the cytoplasm of the host cell. • generally epithelial cells • Basophilic inclusions
Similar to Viral Infections • The methods used to study Chlamydia are those of the virologist rather than the bacteriologist. • The clinical features, pathogenesis, pathology and epidemiology of chlamydial infections are similar to those of viral infections.
Energy Parasites • The cells can synthesize DNA, RNA and protein. • No flavoproteins or cytochromes. • lack of ATP-generating ability • need to obtain ATP from the host cell.
Three species: C. trachomatis C. psittaci C. pneumoniae
Ecology • Chlamydia form two main ecological groups. • Infect only humans • Subgroup A • trachoma, inclusion conjunctivitis, and lymphogranuloma venereum • Zoonotic Infections • Subgroup B • Respiratory tract infections
Zoonotic Infections • transmitted to man • About 100 species of birds are naturally infected with chlamydia. • 71 species of parrots • finches, pigeons, chickens, ducks, turkeys and seabirds.
C trachomatis Trachoma conjunctivitis proctitis urethritis salpingitis Lymphogranuloma venereum C psittaci & C pneumoniae Upper respiratory infection Bronchitis Pneumonia
Chlamydial Morphologies • Elementary body • 0.25 - 0.3 um diameter • electron-dense nucleoid • Released from ruptured infected cells. Human to human • & bird to human. • Reticulate Body • Intracytoplasmic form 0.5 - 1.0 um • Replication and growth. ( Inclusion body ) • without a dense center.
C trachomatis inclusions Glycogen Inclusions
Subgroup A Mammalian parasites Compact inclusions Glycogen synthesized Folates synthesized Sensitive to D-cycloserine Restricted host range Chlamydia trachomatis Subgroup B Primarily bird parasites Diffuse inclusions Glycogen not synthesized Folates not synthesized Resistant to D-cycloserine Broadening of host range Chlamydia psittaci Subgroups
Evolution of Chlamydia • Gram-negative cocci • Facultative intracellular parasites of mammals • Obligate intracellular parasites • Host range restricted to rodents • Restricted virulence (compact inclusions) • Folates synthesized (sulfonamide susceptible) • Glycogen synthesized and deposited in inclusions
Conjunctivitis • Inclusion conjunctivitis: • Transmitted by infectious secretions of the genitourinary tract • autoinoculation • Infantile conjunctivitis: • Acquired in the birth canal -- 5-12 days after birth • most common type of conjunctivitis • Antibiotic prophylaxis: erythromycin, tetracycline.
Trachoma • infection of conjunctival epithelial cells. • subepithelial infiltration of lymphocytes. • Infected epithelial cells contain cytoplasmic inclusion bodies • Cell infiltrations to cornea cause clouding • Trichiasis: abnormal inward growth of eyelashes.
Predisposing factors: • climate - hot , dry • shortage of water • standards of hygiene low Transmitted by flies, dirty towels, fingers, cosmetic eye pencils. Initial infection in childhood mostly by 10-15 years of age.
Trachoma • Almost six million people have become blind and another 540 million almost 10% of the world’s population are at risk
Chlamydia trachomatisClinical disease • lymphogranuloma venereum • nongonoccal urethritis (NGU) • epididymitis • salpingitis • mucopurulent cervicitis • pelvic inflammatory disease (PID) • Reiter's syndrome • neonatal chlamydia
Chlamydia Symptoms In Men • Symptoms usually appear between 7 and 28 days after infection, usually with mild burning when urinating, a more frequent need to urinate, and a white discharge from the penis. Occasionally, blood may appear in the urine. The symptoms occur most frequently in the morning.
Erythematous meatus and urethra with balanitis Hyperlink to original
Nongonococcal urethritis (NGU) - Reiter's syndrome • Swollen, painful right knee in which needle aspiration for synovial fluid was performed (yellow discoloration from the betadine prep) Hyperlink to original site
Lymphogranuloma venereum LGV • 200 reported cases per year. • Incubation period is 5 to 20 days. • Lesion: Transient vesicles on penis or vagina that are often unnoticed and patients do not usually seek medical advice.
Bilateral inguinal adenopathy with overlying erythema R Roberts MD
LGY: "Groove sign" • Pompart's ligament is preserved despite the involvement of multiple inguinal nodes R Roberts MD
LGV: Microscopy • lymph node shows both necrosis and granulomatous reaction (dimorphic necrotizing granulomatous reaction) R Roberts MD
Chlamydia pneumoniae • This bacterium was first recognized in 1983 as a respiratory pathogen, after isolation from a college student with pharyngitis. • Pneumonia or bronchitis, gradual onset of cough with little or no fever. Less common presentations are pharyngitis, laryngitis, and sinusitis.
Incidence • Each year an estimated 50,000 adults are hospitalized with pneumonia in the United States. The overall incidence is unknown.
Transmission • Person-to-person transmission by respiratory secretions. • Risk Groups • All ages at risk but most common in school-age children. By age 20 years, 50% of population have evidence of past infection. Reinfection throughout life appears to be common.
C. pneumoniae Associations • Associated with Heart Disease • infection may be associated with • atherosclerotic vascular disease • Proposed Associations • Alzheimer's diseases, asthma, and reactive arthritis
Adults Conjunctival, urethral, cervical, rectal: Azithromycin 1 gm x 1 dose Doxycycline 100 mg BID for 7 days Ofloxacin 300 mg po BID for 7 days Erythromycin 500 mg QID for 7 days Amoxacillin 500 mg TID 7-10 days Children < 45 kg, urogenital & rectal: erythromycin 50 mg/kg/day in 4 doses for 10-14 days Neonates (ophthalmia, infants born to infected mothers): erthromycin 50 mg/kg/day in 4 doses for 10-14 days Treatment Chlamydia
Chlamydia Antigens Antigens: group specific & species specific • Major outer membrane protein (cysteine-rich) • Eucaryotic cell binding protein Host response: damage to specific tissues
Isolate the organism from infected tissue. Inoculate the yolk sac of seven-day chick embryos Inoculate McCoy human cells. Characteristic cytoplasmic inclusion bodies in infected cells. Laboratory Diagnosis
Immunofluorecent tests • Microimmunofluorescent tests • patients with eye infections • Check tears for the presence of anti-chlamydia antibody. • Direct immunofluorescence • of conjunctive cells with fluorescein - conjugated monoclonal antibody is sensitive and specific. • In neonatal conjunctivitis and early trachoma
Serological diagnosis: • Immunofluorecent tests • Delayed Type Skin Reaction • Antibodies to Family antigen
FREI Test • Delayed-type skin reaction to killed organisms in genitourinary infections
Antibodies to Family antigen • Rising titer of antibody against the chlamydial family antigen in lung infections. • Complement fixation test • Fluorescent antibody test.