Download
1 / 40
400 likes | 681 Views
IPT BOTSWANA EXPERIENCE. Oaitse I Motsamai RN, MW, B Ed, MPH Ministry of Health Botswana 11 th November 2008 Addis Ababa, Ethiopia. OUTLINE. Botswana context Rationale for IPT in Botswana Pilot Current Programme Administration IPT Programme Evaluation. Background of Botswana.

E N D
IPT BOTSWANA EXPERIENCE Oaitse I Motsamai RN, MW, B Ed, MPH Ministry of Health Botswana 11th November 2008 Addis Ababa, Ethiopia
OUTLINE • Botswana context • Rationale for IPT in Botswana • Pilot • Current Programme • Administration • IPT Programme Evaluation
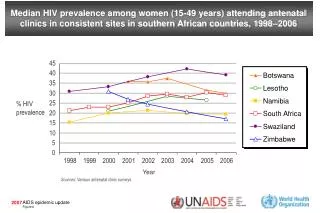
Background of Botswana • Population 1.7 million • HIV prevalence in general population 17% (2004) • HIV prevalence in antenatal women 33.4% (2005) • TB notification rate 514/100,000 (2006) • HIV seroprevalence among TB patients 60-86%
TB Services in Botswana • National TB Program (Disease Control Unit, MOH) • Tuberculosis treatment free and universally available • >600 health facilities provide TB and IPT services • 24 Districts each with TB Coordinator • TB surveillance through electronic TB register
HIV/TB Program Context • Anti-retroviral therapy (ART) has been available since 2001 and is free to all Batswana citizens • Policy on Routine HIV Testing (RHT) introduced 2004 • Under national ART guidelines, TB patients eligible for ART; initiation based on CD4 count • There are 35 ART centers in Botswana
IPT Timeline 1998: Joint WHO/UN Guidelines on HIV/AIDS recommending 6 months of IPT 1999: Formation of an IPT Working Group 2000: Pilot conducted in three districts in to assess feasibility of national scale-up 2001: Pilot completed in April; evaluated in October 2001 2001: National roll out commenced 2003: IPT office established (3 officers) 2004: Complete roll out
Progress of enrolment: 2001-2007 Database rolled out Roll out completed Programme Review Coag signed National office Pilot study
Pilot Study Goals • Assess motivation to undergo testing and accept IPT; • Determine if IPT would increase HCW workload; and • Determine whether HCWs could successfully exclude clients with active disease
Pilot Findings • IPT well-integrated into general clinic services • Acceptable to clients; clients motivated to test by knowledge that HIV interventions (IPT/ART) available • CXR should not be used for ASX patients • Reporting and recoding methods too cumbersome for HCWs Recommendation: Overall, IPT is feasible and should be implemented.
Current Programme • Screen and enroll medically eligible patients referred from VCT/RHT/PMTCT • 6 months self-administered in 6-9 mos. • Monthly follow-up visits • Side effects counseling • TB screening • Compliance • Prescription refill
Eligibility Criteria • Confirmed HIV-infected • 16 years and above • Not currently pregnant • No active TB • No terminal illness • No hepatitis • No history of INH intolerance • No History of TB in the past 3 years
Enrolment • History and physical examination • Exclusion of persons with cough and fever • Client counseling • Monthly review • Side effects assessment • TB screen • Drug re-supply
Enrollment 2001-2007* Registered N=75,235 Eligible n= 73,263 Eligible and started IPT n= 71,541 Completed n=25,075 (33%) Other exclusions (7%) Non-completers n=43,313 (59%) Unknown reason (70%)
Major Challenges • Referral to IPT • Difficult to estimate % eligible captured • Medical Screening • Eligibility • Active TB (prior to and during treatment) • Treatment adherence* (preliminary data, n= 71,541) • Median- 4 follow-up visits • Duration of therapy 98 days • Monitoring and evaluation • High levels of incomplete data • Recording and data entry barriers • Staff turn over: IT no data manager (national)
IPT Staffing • National Level: MOH • National Coordinator • Regional Coordinators (2) • Data officers (3) • IEC officer • Implementation at the district level • Doctors and nurses (MOLG, MOH) • Complementary staff
Support & Supervision • District-level TB Coordinators (DTBCs) placed at District Health Teams • TBCs are supervised by the District Health Teams • District-level activities supervised by TBCs • The national level monitors a sample of facilities on quarterly basis • DHTs are given feedback on their performance • TBCs hold workshops (twice a year) • Training for IPT, TB/HIV surveillance and TB case management, Community TB care for HCWs
Reporting and Recording • Patient out-patient card (pink/blue) • Register and Compliance record • Dispensary Tally Sheet • Patient Transfer form • Monthly Report Form
Other Documents & Database Other IPT Documents: • Training guides: Facilitators’ & Health workers’ • IEC materials: Brochures, video cassettes Electronic Database: • Developed and Funded with the assistance of CDC (BOTUSA) • Rolled out to all 24 districts in November 2005 • Built-in reporting and error functions
Programme Funding • Second-Five year cooperative agreement between CDC and MOH; (2002-2005, 2005-2010) • Ministry of Health provides: infrastructure, drugs & technical support • Clinical staff supported thru Ministry of Local Government O Ministry of Health • CDC provides funds for salaries, training, purchase of equipments; 2001-2007: Over $2 million + technical support
IPT Programme Evaluation • Conducted in May 2008 (external) • Await final report • Reviewed key functions • Referral systems • Medical screening • Adherence • Reporting/recording for M&E • HCW training • Patient counseling • Assessed programmatic implications
Acknowledgements • Botswana National TB Program Staff • CDC Division of TB Elimination • CDC Global AIDS Program/BOTUSA
Caliber Trained • Health professionals: • Doctors • Nurses • Pharmacy Technicians • Health Educators • Social Workers • Non-professionals - Family Welfare Educators - Lay Counselors - Health auxiliary
Challenges Encountered • Overstretched national staff • Inadequate counseling of some clients • Loss of clients who are still on treatment • Lack of clients’ follow up (defaulters) • Transport problems particularly in the districts • High mobility of clients • Wrong addresses given by clients
Challenges Cont’d • Recording and Reporting problems • Incomplete clients’ records • Lack of timely reporting • Personnel • High turnover in districts including TBCs • Weak supervision especially at district level • Training: Continuous re-training of HCW necessary
Botswana Drug Resistance Surveys • Since 1995, 3 resistance surveys done • Fourth resistance survey in progress • Results expected by 4th quarter 2008.
Plans To Prevent Drug Resistance • Emphasis on constant & proper use of the algorithm on screening of clients • Screening of clients at each visit • Thorough investigation of TB suspects • Extensive adherence counseling of clients
IPT as Part of HIV Care and Treatment • Implementation of routine HIV testing from January 2004. • HIV testing of TB patients is routine but so far at 68% • IPT is prescribed in all health facilities by doctors and nurses. • IPT is given as (often first) package of HIV care • Other sources of referral to IPT • PMTCT • VCTs • NGOs • ARV programmes
Integration of TB/HIV services • IPT provides a systematic way to screen PLWH for TB • Policy to provide HAART to HIV-infected TB patients • TB/HIV integrated surveillance rolled out 2005 • TB/HIV advisory body established • TB/HIV care issues in the new TB manual
Achievements • TOTs in all 24 districts (average; 5 per district) • Trained (65%) of all health workers • IPT programme officers at national level • IPT available in all 24 districts and all 636 facilities • Public awareness & uptake has increased • Improved paper based reporting from districts • Computers purchased for all districts
Achievements Continued • Database available in all districts • Designated TB coordinators in almost all districts • Enabled linkage of IPT to TB and ARV databases through the use of national ID • Improved frequency & quality of support visits