Download
1 / 54
550 likes | 764 Views
Terms Used in Relation to Plasmodia. Sporozoite 胞å – The infective stage passed in the saliva of the mosquito and formed inside an oocyst by the process known as sporogony. They are elongated structures measuring about 11µm

E N D
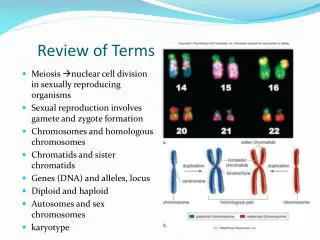
Terms Used in Relation to Plasmodia Sporozoite胞子– The infective stage passed in the saliva of the mosquito and formed inside an oocyst by the process known as sporogony. They are elongated structures measuring about 11µm in length and 1.0µm in diameter. Often they appear curved or bow shaped. Hypnozoite潛隱子– The latent form of the sporozoite seen in P. vivax and apparently responsible for relapses. This is also known as the cryptobiotic phase. Schizont裂殖體– The stage undergoing asexual division by multiple fission or segmentation. Schizonts may be found in the liver cells (pre-erythrocytic schizonts)or in the erythroytes (erythrocytic schizonts). The process is known as schizogony. In malaria this takes place in the human host.
Merozoite裂殖子– The product of division by schizogony. In the electron microscope it appears ovoidal with a cone-sharped end. Two electron dense rhoptries and several micronemes are present at the apical end (see Chapter on Toxoplasma for explanation). Trophozoite營養體– The stage of the asexual form with an undivided nucleus, seen in the erythrocyte. Microgametocyte雄配子– The male gametocyte which produces a number of microgametes. Exflagellation出絲– The process by which microgametes are formed from a microgametocyte. So called because microgametes look like flagella.
Macrogametocyte雌配子– The female gametocyte which produces a single macrogamete. Zygote合子– The fertilized ovum. Ookinete卵動子– The motile stage of the zygote preceding the oocyst stage. Oocyst卵囊體– The zygote after the formation of the cyst wall. In a mature state it is filled with sporozoites. Sporogony胞子生殖– The sexual phase in the life cycle of certain protozoa. In plasmodium this takes place in the mosquito vector. In human malaria only the genus Anopheles is involved.
Romanowsky stain– Mixtures of methylene blue, eosin and methylene azure.Giemsa, Leishman and Wrights are examples of Romanowsky stain. Schuffner’s dots – Pinkish small round stippling seen on P.vivax and P.ovale infected red cells, in Romanowsky- stained films. They appear earlier and in greater numbers in P.ovale than in P. vivax. Maurer’s dots – Coarse and irregular stippling seen onP. falciparum infected red cells in Romanowsky-stained films. Ziemann’s dots – Pinkish small dots sometimes seem in P. malariae infected red cells in Romanowsky-stained films.
Incubation period – The interval between the entry of sporozoites and the first clinical manifestation: P. falciparum 8 to 20 days P. vivax 12 to 15 days P. malariae about 24 days P. ovale about 14 days Pre-patent period – The minimum time between the entry of sporozoites and the first appearance of parasites in the red cells : P. falciparum 6 to 12 days P. vivax 10 to 12 days P. malariae about 21 days P. ovale about 14 days
Parastitaemia寄生蟲血症– A condition in which parasites are present in the blood. This could be symptomatic (often) or asymptomatic (symptomelss parasite carrier). Asymptomatic cases are commonly seen amongst the semi-immunes in the endemic regions. Viremia Paroxysms 發作– Bouts of fever due to the liberation of merozoites during erythrocytic schizogony. Recrudescence再發– Renewed manifestation of infection due to the survival of erythrocytic forms. This is also known as ‘short-term relapse’. Relapse 復發(recurrence) – Renewed manifestation of infection of infection due to the invasion of blood by merozoites from the cryptobiotic phase (hypnozoites). This is the mechanism in P. vivax and P.ovale. This is also known as ‘long-term relapse’.
Latency潛伏期– The duration between the primary attack of malaria and the relapse. There are no parasites in the circulation during this period. Re-infection – Renewed manifestation of infection not due to the original infection but resulting from subsequent fresh infection. Disseminated intravascular coagulation(DIC)散佈性血管內凝血 – A syndrome characterized by the formation of multiple fibrin thrombi in small blood vessels. DIC can occur in P. falciparum infection. Acute respiratory distress syndrome急性呼吸窘迫症– Characterised by rapid breathing and cyanosis發疳. It may occur in P. falciparum infection and carries poor prognosis. Cure, clinical – Cessation of attack and relief of symptoms but not complete elimination of all parasite stages so that relapse can occur.
Cure, radical根源性治癒– Complete elimination of all parasite stages so that relapse can’t occur. Cure, suppressive抑制性痊癒– Elimination of erythrocytic stages by continuous suppressive treatment. Malaria may develop after drug withdrawal. BCRR基本病例再生率– The basic case reproduction rate, i.e. it is the average number of new cases of malaria which will result from one human case in a given place. This may very from over 1,000 to below 1. If the BCRR is below 1 the infection will die out. Stable malaria – Where BCRR is high and practically everyone gets infected. In such populations immunity levels are high and epidemics are less likely. Control is difficult.
Unstable malaria – Where BCRR is generally low and immunity is variable and epidemics are more likely. control is feasible. Sporozoite rate – The percentage of Anopheline females positive for sporozoites on dissection immediately after capture. Spleen rate – The percentage of children between 2-9 years of age showing palpable spleen. Parasite rate – The percentage of persons showing parasites in the blood, generally defined in terms of the age group examined, e.g. children parasite rate or adult parasite rate.
Hypoendemic malaria – Where children of 2-9 years of age have parasite or spleen rates of less than 10%. Mesoendemic malaria – Where children of 2-9 years of age have parasite or spleen rates of 11-50%. Hyperendmic –Where children of 2-9 years of age have parasite or spleen rates of 51-75%. Holoendemic - Where children of 2-9 years of age have parasite or spleen rates of more than 75%. Tolerance – In endemic areas the clinical symptoms are often less for a given level of parasitaemia. Although the mechanism is not clearly understood it is probably related to high immunity.
Genetic susceptibility – P. vivax enters Duffy blood group antigen alleles readily as they appear to act as receptors for merozoites. In Africa Duffy blood groups are rare, therefore, P. vivax is also uncommon. Similarly people with sickle cell trait (HbS/A) are less likely to have fatal P. falciparum infection. Sickle cell trait is common in Africa. Transfusion malaria輸血性瘧疾– Is transmission of parasites via blood from apparently healthy donors. Since the infecting organisms are erythroytic and no sporozoites are involved, the liver cycle does not occur. Congenital malaria先天性瘧疾– If parasites are present in the neonate within 7 days of birth it is regarded as congenital malaria.This is a rare occurrence indicating that the placental barrier and maternal immunity are highly protective normally.
Tropical splenomegaly syndrome (TSS)熱帶脾臟種大症候群– Due to repeated infections and an aberrant immunological response chronic splenomegaly may result. Patients have a high lgM level and antibodies to Plasmodia. It is also known as hyper-reactive malarious splenomegaly. Drug resistance – Parasites may become resistant to any antimalarial drug. Chloroquine resistance to P. falciparum is now widespread in many parts of Asia, Africa and S. America. Resistance is generally graded into 4 catagories: S = no resistance, clearance of asexual parasitaemia occurs within 7 days of initiation of treatment. RI = slight resistance, clearance of parasitaemia as in S but recrudescence occurs after few days. RI I = moderate resistance, marked reduction of asexual parasitaemia, but no clearance. R I I I = absolute resistance, no marked reduction of asexual parasitaemia. Occasionally the parasite numbers may rise.
Quartan malaria nephrosis四日瘧腎病變– P. malariae in some parts of the world produces immune-complex nephritis, leading to nephritic syndrome. Parasite threshold – Level at which parasites become microscopically detectable in the peripheral blood. Fever threshold – Level at which parasite numbers begin to produce fever. This is higher than the parasite threshold. Imported malaria境外移入瘧疾– When injection is acquired outside a specific area and the patient then moves into that area. This kind of malaria is common in W. Europe and the U.S. Introduced malaria – When an imported case introduces infection into a nonendemic area and which leads to local transmission.
Malaria parasites 瘧疾原蟲 Malaria parasites affecting human 瘧原蟲屬 Plasmodium Plasmodium malariae三日瘧原蟲: quartan malaria 四日瘧 Plasmodium vivax間日瘧原蟲: benign tertian malaria三日瘧 Plasmodium ovale : tertian malaria卵圓瘧;三日瘧 Plasmodium falciparum : malignant malaria;三日瘧 (Laverania) 惡性瘧 Plasmodia- monkey
Malaria parasites Geographical distribution P. falciparum :tropical areas, widely P. vivax :wider distribution, tropic or temperate P. malariae: less common P. ovale : less common ; Africa
Malaria parasites Age distribution Young : high mortality and morbidity Adult : low parasitaemia because immune system Pregnant woman : high rate of parasitaemia and clinical symptoms (primigravidae)
Stages of Plasmodium Young trophozoite活動體 Growth trophozoite Schizont 裂殖體 Merozoite 裂殖子 Gametocyte配子 Anophelesminimus Oocyst卵囊體 Sporozoite孢子 Cryptozoite潛隱子
General life cycle of Plasmodium in human host Pre-erythrocytic stage 紅血球前期 Exo-erythrocytic stage Primary exo-erythrocytic Erythrocytic stage 紅血球內期 Gametogenesis 配子體形成
Life cycle of P. vivax andP. ovale Pre-erythrocytic stage Anopheles mosquitoes biting sporozoite into blood stream for about ½ hr sporozoite enter the parenchyma cells of liver pre-erythrocytic schizonts紅血球前期裂殖體 exo-erythrocytic stage and merozoites produce infected cells relapses and merozoites release Cryptobiotic phase (hypnozoites) 隱眠小體
Life cycle of P. vivax andP. ovale Erythrocytic stage Merozoites enter RBC to form the parasitic vaculoe Trophozoite transformate from merozoite Trophozoite maturation : haemoglobin digestion (haemozoin) (malaria pigment)瘧疾色素
Life cycle of P. vivax andP. ovale Erythrocytic stage Schizogonic cycles schizogony formation daughter merozoites Gamatocytes formation microgamatocytes雄配子 macrogamatocytes雌配子
Life cycle of P. vivax andP. ovale Sexually stage (Vector stage) Exflagellates and macrogamatocytes formation Zygote formation Ookinete formation : 4-6 hr卵動子 and penetrate into midgut wall Oocyst formation Sporozoites develop from sporoblasts胞子胚細胞 Sporozoites migrate to salivary gland
Apical complex Rhoptries : enzymes Micronemes Nucleus
Life cycle of P. malariae Similar to P. vivax persistence infection due to the survival of the blood forms (erythrocytic stages) in small numbers (30 years) not due to hypnozoites潛隱子
Life cycle of P. Life cycle of P. falciparum Asexually stage vector mosquito biting pre-erythrocytic stage sporozoites develop in liver cells merozoites discharge into blood stream erythrocytic stage merozoite invade into RBC re-cyclic invasion of RBC with merozoite
Life cycle of P. Life cycle of P. falciparum Sexually stage some merozoites transformed into gametocytes macrogametocytes and microgametocytes vector mosquitoes blood meal feeding exflagellates and macrogametes forming in midgut zygotes formation oocysts formation sporozoites releasing
Malaria parasites Clinical aspects Cold & hot response during fever phase Merozoite & Endogenous pyrogen release into blood stream Cold stage : 30-60 min. Hot stage : 1-4 hr Sweating stage : 1-2 hr Atypical case: paroxysms of fever don’t occur diarrhoea, headache, abdominal pain, jaundice, hallucinations, respiratory or renal symptoms
Malaria parasites Clinical aspects P. falciparum infection produce serious complications Cerebrain malaria腦性瘧疾: brain Black-water fever: massive haemoglobinuria大量血紅素尿症 Acute respiratory distress syndrome呼吸窘迫 Hyperpyrexia 極高熱 Severe gastrointestinal symptoms Hypotension Algid malaria (shock) Diagnosis should be established early
Malaria parasites Pathophysiology fig. 54 Complex changes changes RBC function dysfunction of several organs liver failure Death pulmonary edema cerebral edema haemorrhage insufficiency drugs toxicity Tumour necrosis factor (TNF)
Malaria parasites Diagnosis Blood semear diagnosis thick semear: light infection thin semear: species diagnosis DNA probes detection Serological tests IFA, IHA, ELISA epidemiological studies
Malaria parasites Treatment Anti-malaria drugs treatment quinine奎寧 chloroquine氯奎寧 primaquine proguanil pyrimethamine sulphadoxin dapsone Malignant tertian malaria antiparasitic drugs supportive measure
Malaria parasites Treatment of uncomplicated falciparum malaria p. 67
Malaria parasites Treatment of complicated falciparum malaria p. 68
Malaria parasites Supportive measures
Malaria parasites Treatment of vivax and ovale malaria
Malaria parasites Treatment of malariae malaria
Malaria parasites Chemoprophylaxis 化學預防法 Pyrimethamine : 25 mg / weekly Proguanil: 100 – 200 mg/ daily Chloroquine : 300 mg / weekly; 1 week before & 4 weeks after Pyrimethamine 25 g + suylfadoxine 500 mg/ weekly Pyrimethamine 12.5 mg + sulphone 100 mg / weekly Mefloquine 250 mg / weekly Doxycycline 100 mg / daily
Malaria parasites New antimalarial drugs Mefloquine hydrochloride: Qinghaosu: Halofantrine : phenanthrine + methanol
Malaria parasites Prevention and control Vector control : Insecticide residue effects Genetic modified mosquitoes Patients rescue : Anti malaria drug
Babesia spp Babesiosis 巴貝斯蟲病; 梨漿蟲病 General biology World wild distribution Very important parasite in livestock and domestic animal Tickas a vector ; no human transmission Sporadic cases in humans: Europe, America, Russia Babesia bovis(bovine牛); B. microti(murine鼠) Splenectomised脾臟切除persons are more infected