Download
1 / 26
260 likes | 361 Views
DEALING WITH DISRUPTIVE FACULTY BEHAVIOR. “Surgeon Arrested After Throwing Fit”. Oakland, CA March 26, 2006 A neurosurgeon was wrestled to the floor by sheriff’s deputies outside the operating room after he threw a fit because he had to wait for instruments to be sterilized, authorities say.

E N D
“Surgeon Arrested After Throwing Fit” Oakland, CA March 26, 2006 A neurosurgeon was wrestled to the floor by sheriff’s deputies outside the operating room after he threw a fit because he had to wait for instruments to be sterilized, authorities say. USAToday.com
OBJECTIVES • to explore the impact of and possible causes of difficult behavior • to describe the process of intervention • to identify resources to assist in managing challenging faculty • to discuss possible prevention/proactive strategies
Measure performance Take Corrective Action THE PYRAMID APPROACH 6 Manage performance 5 4 Providefeedback 3 2 Set and communicate expectations 1 Appoint excellent faculty/staff Sheff, MD and Sagin, MD
DISRUPTIVE BEHAVIOR • “personal conduct, whether verbal or physical, that negatively affects or that potentially may negatively affect patient care”.
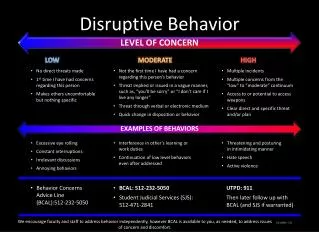
EXAMPLES OF UNACCEPTABLE BEHAVIOR • Profane/disrespectful language • Outbursts of rage • Racial or ethnic jokes • Demeaning/intimidating behavior • Sexual comments or innuendo • Throwing objects • Criticizing other professionals in public
UAB Code of Conduct for Professional Behavior
2004 SURVEY • >95% of physician execs encounter disruptive behavior on a regular basis • Of the 1600 respondents, 1 in 3 said they observe problems with physician behavior either weekly (14%) or monthly (18%) • Weber, D.O. (2004) Poll Results: Doctors’ disruptive behavior disturbs physician leaders. The Physician Executive, 30, 4, 6-10
IMPACT • Affects patient care and safety • Disrupts facility operations • Creates hostile work environment • Lowers community’s confidence
WHY ARE SOME FACULTY CHALLENGING? System level issues Personality Issues Lack of Skills Medical/Mental Illness Work Stress Syndromes Remember: Difficult docs are often docs in difficulty
WHAT CAN WE DO? • Undertake a cultural transformation • Devote adequate time/resources • Provide extensive education/training • Develop thorough policies/bylaws • Enforce policies
INTERVENTION • Goal is to ensure that faculty • Owns responsibility for behavior • Commits to improve it • Takes active steps • Schedule follow up visit
Collegial “doc in the box” ESCALATING INTERVENTIONS
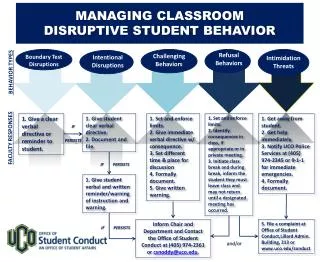
PLANNING THE INTERVENTION • Who? 1-2 people • Where? Private setting • When? As close to event as possible • What are faculty’s likely responses? • What is plan B? • How will you monitor any changes?
Identify the problem behavior Refer to policy Deflect excuses Constantly refer to data Be persistent Keep time limited Close with faculty commitment Explain documentation procedure PRACTICE THE INTERVENTION
2 FORMULAS • F – State Facts I - State Impact R - Give Respect R – Make Request • U - Understand other’s point of view 1st S - State your Situation A - Alternative Action
Resources a. professional assessment b. human resources c. legal/administrative counsel d. educational materials
PHYSICIAN RESOURCE OFFICE UAB Highlands 930-7680
RESOURCES AVAILABLE THROUGH HR • HR Relations – consultation, policy interpretation • Dr. Pam Burks – facilitated conversations • The Resource Center – free, confidential counseling for faculty and their family members
Educational Materials • Difficult Conversations, by Douglas Stone, et al • Crucial Conversations, by Kerry Patterson, et al • Dealing With Different, Diverse, and Difficult People, -audio series, by Barbara Braunstein
Possible Recommendations • Individual counseling/coaching • Educational event/workshop • Workplace “monitor” • Regular feedback meetings • 360° surveys for all faculty • Psychological testing • Inpatient evaluation • Corrective action
PREVENTION/PROACTIVE STRATEGIES • New faculty orientation • Educate regarding Code of Conduct • Annual performance evaluation • 360° feedback surveys • Clearly communicate goals/expectations for Dept/Div/faculty member Be consistent
Universal Code of Conduct Planned Implementation Compliance Monitoring Non Retaliation Provisions Code Enforcement Resources/Options Oversight Committee Preventive Strategies IN SUMMARY
Case 1 A faculty member constantly interrupts you during meetings and openly criticizes your suggestions. • How would you handle this?
Case 2 QZ has been a productive faculty member in your division for 5 years. However you have received numerous complaints from both staff and patients that he is rude and demeaning, and the complaints are increasing. • What would you do? • Would it make a difference if he is tenured vs non tenured?