Download
1 / 4
50 likes | 404 Views
TRANSITIONAL CELL CARCINOMA IN DOGS. 로얄벳 동물병원 원 장 김희용.

E N D
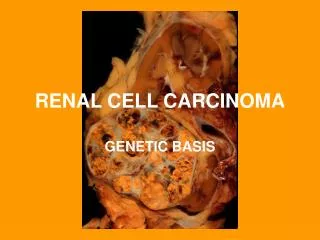
TRANSITIONAL CELL CARCINOMA IN DOGS 로얄벳 동물병원 원장 김희용
Transitional cell carcinoma (TCC) is the most common urinary tract tumor in dogs and research suggests that it may becoming more common. The main differential diagnosis and also the most common `misdiagnosis` is chronic recurrent cystitis. This excellent article gives an overview of the current diagnostic and therapeutic options.Generally, TCC occurs in older dogs (mean age 11 years) and it occurs in females more frequently than in males. The increasing incidence of TCC may be related to pet obesity, use of topical pesticides for fleas/ticks, or environmental pollutants. (Mutsaers AJ, Widmer WR, Knapp DW. Transitional Cell Carcinoma. J Vet Intern Med 2003: 136-144).
Diagnosis Urinary tract tumors should be considered in any dog with hematuria, stranguria or polakyuria that does not rapidly and completely respond to appropriate antibiotic therapy. Secondary urinary tract infections are common with TCC. The veterinarian should not exclude TCC from the rule-out list based on a positive urine culture or an improvement in clinical signs while on antibiotics. The other rule-outs for recurring hematuria or dysuria include urinary calculi, resistant infections, anatomic defects, tumors other than TCC and rarely foreign bodies. Initial evaluation for hematuria/dysuria should include: urinalysis, urine culture, rectal palpation to evaluate urethra/prostate and abdominal radiographs. Further evaluation might include CBC/chemistries, abdominal ultrasound, contrast studies, cystoscopy/vaginoscopy or surgery. Urine screening test A new urine screening test for transitional cell carcinoma is now also available (V-BTA test; Polymedco Inc; Redmond, Wash.) The test is a latex agglutination assay for glycoproteins released from the basement membrane of the bladder affected by cancer. The test has a sensitivity of 90 percent and a specificity of 78 percent. Interference with the test (causing false positives) occurs with marked glucosuria (4+), heavy proteinuria (4+) or pyuria/hematuria (>30-40 WBC or RBC/hpf). Therefore a negative test has an accurate negative predictive value of 95 percent, but a positive test result would mean that further evaluation is indicated to rule-in or rule-out neoplasia. Definitive diagnosis of TCC requires a histopathologic evaluation of tissue collected by catheter biopsy (usually ultrasound-guided), cystoscopy or cystotomy. Ultrasound also provides information regarding possible metastasis to lymph nodes or other organs, and provides information regarding possible surgical resection of the tumor.
If ultrasound is not available, or of limited usefulness due to tumor mineralization or distal uretheral involvement, contrast cystourethrogram is indicated. TCC most commonly affects the trigone of the bladder and therefore curative surgical resection is often not possible due to ureter involvement. Therefore, understanding anatomic involvement prior to surgery is very useful for therapy and prognosis. Therapy 1. Surgery: Whenever possible, surgical resection with margins is ideal, but this is usually limited to the situation of bladder apex tumors. Debulking of vaginal urethral tumors is sometimes necessary to maintain ability to urinate and relieve discomfort. 2. Chemotherapy: TCC is generally poorly responsive to chemotherapy. Although some response has been reported to doxorubricin/cyclophosphamide and doxorubricin/platinum combinations. NSAID therapy with piroxicam has led to partial remissions as well as rare complete remissions. Unlike chemotherapy agents, piroxicam appears to cause apoptosis of TCC cells. Piroxicam is a strong NSAID and so may cause gastrointestinal irritation. This author does not automatically use a histamine blocker or sucralfate concomitantly, but will if clinical signs of nausea, inappetance or melena warrant it. I never use prednisone concurrently with piroxicam due to the marked increase of gastrointestinal ulcers when using these drugs together. Source: Lisa Ann Dzyban (2004): Recurring cystitis or something else? In: DVM Newsmagazine June 1, 2004; www.dvmnewsmagazine.com/dvm/