Download
1 / 23
230 likes | 365 Views
2 Key Valuation Issues I. The Value of Shares for Physician Buy-in and II. Valuing Compensation Relationships in Under Arrangement Models 14 th Annual Ambulatory Surgery Center Conference October 20, 2007 Presented By: Stephan Peron, VMG Health, LLC Curtis Bernstein, HealthCare Appraisers, Inc.

E N D
2 Key Valuation IssuesI. The Value of Shares for Physician Buy-in and II. Valuing Compensation Relationships in Under Arrangement Models14th Annual AmbulatorySurgery CenterConferenceOctober 20, 2007Presented By:Stephan Peron, VMG Health, LLCCurtis Bernstein, HealthCare Appraisers, Inc.
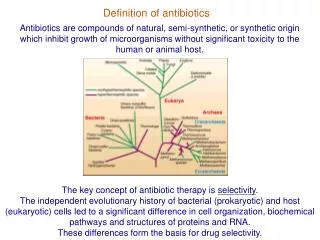
Definition of FMV In Revenue Ruling 59-60, the Internal Revenue Service defines fair market value as “the amount at which property would change hands between a willing seller and a willing buyer when the former is not under any compulsion to buy and the latter is not under any compulsion to sell and when both have reasonable knowledge of the relevant facts.”
Valuation Guidance from the IRS Revenue Ruling 59-60 also states that all relevant factors should be considered, including the following: • The nature of the business and history of the enterprise from its inception; • The overall economic outlook, and the condition and outlook of the specific industry in particular; • The book value of the stockholders’ equity and the financial condition of the business; • The earning capacity of the company; • The dividend-paying capacity of the enterprise; • Sales of the stock and the size of the block to be valued; and • The market price of publicly traded stock of corporations in similar industries or lines of business.
Basic Valuation Theory Time Value of Money • If I invest $1,000 today at 10% annually, I will earn $100 next year, $110 in year 2, etc. • The inverse is true – if I expect to earn $100 next year, $110 in year two, etc. from an investment in which I expect to earn 10%, I would be willing to pay $1,000 today for that investment
Conversion to a Multiple The current FMV of a non-controlling interest in an ASC is currently trading between 3.0 and 4.5 times adjusted* EBITDA less debt. • Reconciliation to “Basic Valuation Theory” • An investor would expect a 22% to a 33% return annually on an investment in a non-controlling interest in a particular ASC. *Adjusted based on post DRA revenue
The Value of Shares for Physician Buy-in Considerations Selling Equity to Physicians • Current ownership structure • Percentage equity available for sale • Availability of existing shares for sale • Sale of new shares • Maximum and minimum percentage available per physician • Return on investment (ROI) of equity investment • OIG and IRS regulatory requirements related to valuation • ASC safe harbors of the Anti-Kickback Statutes • Term of existing operating agreement • Management of partnership • Buyout provisions and covenants not to compete • Value of equity at minority and control level
Valuation Issues • Regulatory requirements for valuation (OIG and IRS) • Fair market value opinion vs. pricing analysis • Pricing analysis using limited valuation methods • Fair market value opinion using complete valuation process • Timing and cost considerations • Reasonable consideration of non public minority level equity
Valuation Issues Specific to ASCs • Physician ownership makeup or lack thereof • Physician risk is the most important risk factor in ASC valuation • Case volume, mix, and reimbursement • Change in volume and reimbursement per case • Diversification (e.g., # of surgeons, number & type of specialties, payors) • Nature of payor contracts – “out of network” business • Market reimbursement risk analysis • Ability to generate sustainable cash flow and distributions
Valuation Issues Specific to ASCs • Financial leverage, working capital, and capital expenditures • Quality and age of facility and equipment • Opportunity for expansion (rooms, surgeons) • Competent management • Barriers to entry (e.g., CON) • Terms of operating agreement • Divesture required upon retirement, relocation, and inactivity • Restrictive covenants
Valuation MethodologyDecision Tree ASC Attributes
Valuing Minority Interests • Simply states: Interests providing absolute control (i.e., greater than a 50% interest whereby key aspects of control are not diminished by governing documents or otherwise) are worth more than interests which do not have the same control rights • Control granted by the governing documents (examples on next slide) • Concept of “effective” control – physicians control with their feet and their hands • Valuation Guidance: absence of control adjustments in financial projection (preferable approach) or application of minority interest discount (reliance on published studies or other more difficult to quantify and support)
Valuing Minority InterestsMatters Subject to Control • Capital calls • Admission of new investors • Borrowings greater than a certain amount • Acquisition of equipment greater than a certain amount • Selling, assigning or otherwise disposing or encumbering assets • Entering into material contracts • Management agreement contracts (assigning/cancelling) • Selling, liquidating, or merging the entity • Changing the core governing documents • Typical ASC ownership agreement are very friendly to the minority shareholder • Note: Physicians display a certain level of control regardless of ownership interest level
Stark - Phase III • Centers for Medicare and Medicaid Services (“CMS”) posted the final Stark Phase III on August 27, 20007 (Federal Register September 5th) • With respect to indirect compensation arrangements, CMS explains in the final rule that the relationship between the physician and his or her physician organization is disregarded and the physician “stands in the shoes” of his or her physician organization. • CMS states, “many arrangements that may not have met the definition of an ‘indirect compensation arrangement’ under the Phase I and Phase II analysis will constitute direct compensation arrangements that must satisfy the requirements of an exception in order for the physician to make DHS referrals to the entity furnishing DHS.” • RESULT: Consult your regulatory attorneys to assist with the legal issues associate with an under arrangement structure
Case Study: “Under Arrangements” Business Model • Primary Model, can vary depending upon desired structure and state-specific regulations • Hospital contracts with a separate legal entity formed to provide turnkey surgical management services to Hospital’s outpatient department (i.e., separate legal entity is not an outpatient surgical center, but rather, a management company) • Management company, “NewCo,” can be jointly owned by Hospital and Physicians or 100% physician owned • NewCo would provide facility services to the hospital pursuant to a written agreement • The Hospital would bill for those services under the Hospital’s name and provider number • Hospital directly compensates NewCo for its services in an amount that is reasonable based on the going rate charges in the community to other entities that provide comparable services
Case Study: “Under Arrangements” Business Model - Advantages • Allows hospital to offer seamless outpatient surgical services to patients in collaboration with physicians within the community, enhancing quality of care and patient satisfaction • Increased efficiency & cost controls: MDs generally have a demonstrated ability to offer cost-effective services on an outpatient basis • Creates an alternative mechanism for hospitals and physicians to offer outpatient services to patients beyond the standard free-standing, independent surgery center • Preserves hospital’s ability to leverage upon existing payor contracts • Expansion of current services through access to needed capital: allows hospital to preserve capital for other equally important projects • Creates a mechanism to recruit and retain physicians • Creates an opportunity for physicians to participate with hospital and earn economic returns in exchange for assuming certain business and financial risk
“Under Arrangements” Business Typical Model • HOSPITAL OUTPATIENT DEPARTMENT • Maintains patient relationship, QA, and Medical Records • Holds managed care contracts and performs billing & collection function • Contracts with NewCo for the • provision of “turnkey” services • Pays NewCo a management fee • “NEWCO” JOINT VENTURE • Purchases equipment and supplies; employs staff • Can be jointly owned by hospital and physicians or 100% MD owned • Contracts with hospital for the provision of “turnkey” outpatient surgical services • Receives management fee from hospital, which is comprised of reimbursement of reasonable and necessary operating costs as well as a market rate of return
Case StudyFacts: • Small rural area of about 50,000 population; • One local hospital with outpatient surgical volumes of approximately 4,000 annually; • Estimated income to hospital - $1,00,000 annually; • Physicians threaten to start own ASC;
Case StudyFreestanding ASC model • Hospital and physicians joint venture the ASC. • Who determines who gets what percent? • Hospital is required to over build to meet the needs of certain physicians (“politics” says Hospital’s CEO) • New Center is required to get new Medicare number and negotiate new payor contracts • Center and Hospital compete in same market – increased competition leads to ASC getting lower reimbursement than Hospital. • Resulting income = ($350,000) in year one and making a slight profit by year four
Case StudyUnder Arrangement Model • Hospital owns department; • Hospital and physicians joint venture management company; • Hospital outpatient department already build out – no additional build out capital expenditure necessary; • Hospital contracts in-place – no delay in payments and no renegotiation; • Hospital continues to earn a significant profit, actually exceeding historic profits from its outpatient surgery business by year four; • Under arrangement company only earns a 10% profit but returns to investors equal to 30% annually. • Result: Hospital retains income that can be used to fund non-profitable business such as the ED, Labor & Delivery, etc. • Result: Physicians have their ownership in outpatient surgical business and make profit similar to that made in their own business.
Methodology for Establishing FMV • Clearly define which entity will provide which service • Determine Managers estimated cost of providing the turnkey service; differentiate fixed from variable; perform sensitivity analysis over a relevant range of volume assumptions • Mirror costing assumptions to proposed level of payment (i.e., one weighted average per case fee vs. payment designed around specific procedures) • Research similar arrangements in the marketplace; research market rates of return for comparable operating entities and leasing companies; apply operating margin return to manager’s fully loaded cost per case figure (example on next page) • Examine rates of return for each party to the agreement over a relevant range of volume assumptions; assess for reasonableness and equity
Methodology for Establishing FMVPer Case Fee Calculation (Simplified Example) Assume: fully loaded cost per case (including debt service on equipment) = $1,000 / case Assume: Market research indicates that profit margins reasonably range between 20% and 30% Per Case Fee calculated as (Cost Per Case) / 1 – Operating Margin) Low: $1,000 / ( 1 - 0.2) = $1,250 (i.e., $250 represents a 20% operating profit margin on $1,250 in “revenue” to manager) High: $1,000 / (1 – 0.3) = $1,429 (i.e., $429 represents a 30% operating profit margin on $1,429 in “revenue” to manager) Depending upon scope of services provided, look at RBRVS reimbursement as a measure of reasonableness CANNOT BASE “PER CASE” PAYMENT ON HOSPITAL’S REIMBURSEMENT: FMV WOULD DICTATE THAT HOSPITAL PAY A MARKET RATE OF RETURN FOR SERVICES PURCHASED AND NOTHING MORE . . . .
Stephan Peron, AVA VMG Health, LLC Three Galleria Tower 13155 Noel Road, Suite 2400 Dallas, Texas 75240 (214) 369-4888 stephanp@vmghealth.com Curtis Bernstein, CPA/ABV, CVA, MBA HealthCare Appraisers, Inc. 858 Happy Canyon Road, Suite 240 Castle Rock, CO 80108 (303) 688-0700 cbernstein@hcfmv.com