Download
1 / 55
550 likes | 790 Views
Generation and reading of the 12 lead ECG. AWC Chow. The 12 lead ECG. Advantages Common clinical tool Independent marker of cardiac disease Non-invasive Rapid information acquisition Cheap Gold standard for arrhythmia management. The 12 lead ECG. Disadvantages Average of potentials

E N D
The 12 lead ECG Advantages • Common clinical tool • Independent marker of cardiac disease • Non-invasive • Rapid information acquisition • Cheap • Gold standard for arrhythmia management
The 12 lead ECG Disadvantages • Average of potentials • Limited resolution • Snapshot of activity • Electrical and not haemodynamic data
Non-specialised atrial tissue Left bundle Anterior superior fascicle Right bundle Posterior inferior fascicle
- +/- +
History of the ECG • 1842 -Carlo Matteucci shows that an electric current accompanies each heart beat. • 1874 - Sanderson and Page record the heart's electrical current with a capillary electrometer • 1887 - British physiologist Augustus D. Waller publishes the first human electrocardiogram. • 1901 - Einthoven develops the string galvometer • 1910 – Eithoven’s triangle
Theoretical consideration • Myocytes have a resting potential • Transmembrane flux create voltage difference - activation • Cellular coupling cause rapid deploarisation • Ionic flux seen ECG deflections
Theoretical considerations • Resting state - no potential/field change • Depolarisation - boundary potential change • Represented as a dipole/vector • Restitution of polarity: repolarisation
Theoretical considerations • Greater muscle mass • Larger potential change • Larger voltage changes of ECG • Direction of activation dependent on • Site of initiation • Specialised conduction system distribution • Anatomical considerations • Barriers (scar, valves) • Muscle mass
RA LA I II III RL LL
aVR +210 aVL -30 I 0 II +60 III +120 aVF +90
PR T P QT QRS
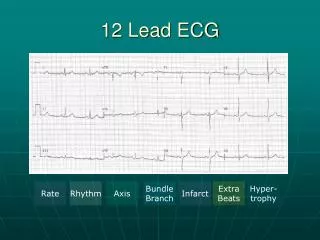
Diagnostic criteria for LVH There are many different criteria for LVH. • Sokolow + Lyon (Am Heart J, 1949;37:161) S V1+ R V5 or V6 > 35 mm • Cornell criteria (Circulation, 1987;3: 565-72) SV3 + R avl > 28 mm in men SV3 + R avl > 20 mm in women • Framingham criteria (Circulation,1990; 81:815-820) R avl > 11mm, R V4-6 > 25mm S V1-3 > 25 mm, S V1 or V2 + R V5 or V6 > 35 mm, R I + S III > 25 mm • Romhilt + Estes (Am Heart J, 1986:75:752-58) Point score system
Causes of RBBB • normal finding in children and tall thin adults • right ventricular hypertrophy • chronic lung disease even without pulmonary hypertension • anterolateral myocardial infarction • left posterior hemiblock • pulmonary embolus • Wolff-Parkinson-White syndrome - left sided accessory pathway • atrial septal defect • ventricular septal defect
Causes of LBBB • left anterior hemiblock • Q waves of inferior myocardial infarction • artificial cardiac pacing • emphysema • hyperkalaemia • Wolff-Parkinson-White syndrome - right sided accessory pathway • tricuspid atresia • ostium primum ASD
ECG Analysis • Rate 60-100b/min • Rhythm SR • PR <200ms • QRS <120ms • Axis -30 to +120 • QT interval <500ms • ST segment