Download
1 / 37
630 likes | 1.34k Views
TCGA: Past, Present & Future. July 11, 2013 Kenna Shaw, Ph.D. Director TCGA Program Office National Cancer Institute. TCGA: Core Objectives. Launched in 2006 as a pilot and expanded in 2009, the goals of TCGA are to: Establish infrastructure for effective team science

E N D
TCGA: Past, Present & Future July 11, 2013 Kenna Shaw, Ph.D. Director TCGA Program Office National Cancer Institute
TCGA: Core Objectives Launched in 2006 as a pilot and expanded in 2009, the goals of TCGA are to: • Establish infrastructure for effective team science • Develop a scalable “pipeline” • Demonstrate the feasibility of a large-scale, high throughput approach to identifying the molecular ‘parts-list’ • Make the data publicly and broadly available to the cancer community while protecting patient privacy
TCGA: Timeline Analysis Completion Pilot Project Expansion 2005 2006-2009 2015-2016 2010-2014 GBM Report Ovarian Report ARRA Funding Rare Projects Initiated 9 tumor types closed 10,000 cases complete NCAB Report • Pilot Projects: GBM and Ovarian carcinoma (~500 cases ea.) • Establish infrastructure for effective team science • Develop a scalable “pipeline” • Demonstrate the feasibility of a large-scale, high throughput approach to identifying the molecular ‘parts-list’ • Make the data publicly and broadly available to the cancer community while protecting patient privacy • Expansion 2010 to 2014: • Add 25-35 tumor types • Enhancement of sample acquisition & program staff • Add Genome Data Analysis Centers • Publish “Benchmark Marker Papers” • Established FFPE protocols • Completely characterize 10,000th case • Analysis Completion 2015-2016: • Finish marker papers on rare & “challenging-to-accrue” tumors • Complete Pan-Cancer Analysis • Broader sharing of tools, analytical methods
TCGA: “No Platform Left Behind” • Multiple data types • Clinical diagnosis • Treatment history • Histologic diagnosis • Pathologic report/images • Tissue anatomic site • Surgical history • Gene expression/RNA sequence • Chromosomal copy number • Loss of heterozygosity • Methylation patterns • miRNA expression • DNA sequence • RPPA (protein) • Subset for Mass Spec 25* forms of cancer glioblastoma multiforme(brain) squamous carcinoma(lung) serouscystadenocarcinoma(ovarian) Etc. Etc. Etc. Biospecimen CoreResource with more than 150 Tissue Source Sites 6 Cancer GenomicCharacterization Centers 3 GenomeSequencingCenters 7 Genome Data Analysis Centers Data Coordinating Center
TCGA Tumor Types • Hepatocellular • Lower Grade Glioma • Lung adenocarcinoma* • Lung squamous* • Melanoma • Ovarian serous cystadenocarcinoma* • Papillary kidney • Pancreas • Prostate • Sarcoma (dedifflipo, UPS, leiomyosarcoma) • Papillary Thyroid* • AML • Breast Ductal* • Breast Lobular/Breast Other • Bladder (pap and non-pap) • Cervical adeno & squamous • Colorectal* • Clear cell kidney* • DLBCL • Endometrial carcinoma* • Esophageal adeno & squamous • Gastric adenocarcinoma • GBM* • Head and Neck Squamous* Red- Pilot tumors; *- Reached 500
Rare Tumor Project (Approved March 2012) • Adrenocortical Carcinoma* • Chromophobe kidney* • Mesothelioma • Paraganglioma/Pheochromocytoma • Uterine Carcinosarcoma* • Thymoma • Uveal Melanoma • Testicular Germ Cell • Cholangiocarcinoma • Diffuse Large B Cell Lymphoma
Tumor Project Progress * Manuscript submitted or published Analysis underway * * Sample acquisition phase * * * * * * * Rare tumor project * Only accepting AA cases/500 target reached
Sample Criteria Limit ‘Askable’ Questions • Primary,adult tumors (except for melanoma and triplets) • Malignant (no in situ cases) • Snap frozen, <60min from clamp to LN2 • ~ 50 mg (biopsies starting to be feasible) • Pathology review of tissue sent to TCGA • No more than 20% necrosis ; ≥ 60%* tumor cells • No prior treatment • Matchedsource of germline: Blood (buffy coat/white cells)/saliva or skin for liquid tumors • Clinical annotation; but not pre-analytic variables • IRB approval for use in TCGA; proactive consenting for genomic studies • MTA w/out retention of IP 10,000 10
TCGA: What’s in a Core Data Set? Data from Tissue Source Sites Data Generated by GCCs &GSCs Core Data Set • Synopic path report • Histology images • Required clinical data • Whole exome • SNP 6.0 array • mRNAseq • miRNAseq • Methylation array • Complete path report • Paired metastatic samples • Double normals • Treatment data • 50X WGS • 8X WGS • Methylseq • RPPA (May not apply to GBM/Ovarian cases collected during the pilot phase)
TCGA: The Pipeline for Comprehensive Characterization Tissue Sample GDAC Pathology QC Sequencing Data Storage at DCC & CGHub Integrative Analysis DNA & RNAIsolation, QC Expression,CNA & LOH,Epigenetics Comprehensive Characterization of a Cancer Genome 3 months – 2 years SNP 6.0 ~45d ~90d Methylation ~60d miRNAseq ~105d mRNAseq ~120d ~12-24 months DNAseq Exome ~180d
TCGA: Lessons Learned from the Data Pathway Analyses #1: It’s About Pathways and Integrated Analyses
TCGA: Lessons Across CancersLearned from the Data #2: Generating the comprehensive parts list will require many tumor types.
TCGA: Lessons Learned from the Data ultramutators Female GBM 2.5y Alive and Well M. Lawrence & G. Getz/Broad Institute
TCGA: Lessons Learned from the Data M. Lawrence & G. Getz/Broad Institute
TCGA: Lessons Learned from the Data M. Lawrence & G. Getz/Broad Institute
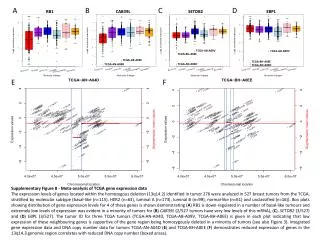
Genomic Data Complements Histopathologic Dx 1q amplification 24% of high-grade endometrioid tumors cluster with serous tumors (serous-like) • Andrew Cherniack, Broad
TCGA: Lessons Learned from the Data #3: Publicly accessible, high-quality data is necessary but not sufficient to build a community of thousands of users.
Where to find TCGA Sequence Data • Moved from Short Read Archive (SRA at NCBI) to UCSC • Open for downloads as of January 2012 • Ready for 2 petabytes now, 5Pb (5 x 1015) total by 2014 • General Parallel File System, Dual RAID 6 subsystems, Redundant I/O paths • Currently holds >30,000 files • Co-location opportunities in same data center for groups who want to compute on the data • User support: support@cghub.ucsc.edu https://cghub.ucsc.edu
Ongoing Pipeline Analysis Available http://gdac.broadinstitute.org
Analysis Portal Examples: MSK’s cBio Phenotype & Clinical tracks Cancer tracks http://www.cbioportal.org/public-portal/ Are there differences in survival? I’m interested in “X” gene pathway in colorectal cancer… I’m interested in Patient TCGA-XX-YYYY “I’m curious about this specific region in detail” LBL’s BioSig Image Analysis Tool http://tcga.lbl.gov/biosig/tcgadownload.do UCSC’s Cancer Genome Browser http://genome.ucsc.edu/ MSKCC’s cBIO Genomics Portal http://www.cbioportal.org/public-portal/ MSKCC’s cBIO Genomics Portal http://www.cbioportal.org/public-portal/
TCGA: The Pipeline for Comprehensive Characterization Tissue Sample GDAC Pathology QC Sequencing Data Storage at DCC & CGHub Integrative Analysis DNA & RNAIsolation, QC Expression,CNA & LOH,Epigenetics Comprehensive Characterization of a Cancer Genome • Model Informed Consents • Novel contracting methods to incentivize quality • FFPE sequencing/array protocols • Benchmarking datasets • Innovating cancer genomes analysis • Cross-tumor discovery • Innovating Data storage/release policies • New data standards (e.g. cancer .vcf) • FFPE isolation protocols • Remote pathology review • Reduction of batch effects
Genomics-Driven Cancer Medicine: Guiding Principles for the Center for Cancer Genomics Principle #1: Molecular pathways involved in tumor survival and progression are often activated by genetic alterations. Garraway, J. Clin. Oncol., 2013
Genomics-Driven Cancer Medicine: Guiding Principles for the Center for Cancer Genomics Principle #1: Molecular pathways involved in tumor survival and progression are often activated by genetic alterations. Principle #2: Anticancer agents targeting many oncogenic pathways have entered clinical trials. Garraway, J. Clin. Oncol., 2013
Genomics-Driven Cancer Medicine: Guiding Principles for the Center for Cancer Genomics Principle #1: Molecular pathways involved in tumor survival and progression are often activated by genetic alterations. Principle #2: Anticancer agents targeting many oncogenic pathways have entered clinical trials. Principle #3: Genomics technologies enable robust tumor genomic profiling in the clinical arena.
Center for Cancer Genomics (CCG)Portfolio • Signature CCG projects • Driven by CCG • Address large questions by coordinating across studies/divisions • e.g. 10,000 cases from CCG, DCTD, DCEG, CCR, DCCPS…. • Strategic partnerships with other NCI Divisions • Share bio-informatic tools/pipelines • Share SOPs for genomic analysis • Provide genome data quality assurance
Strategic CCR partnerships with other NCI Divisions FFPE Samples from Clinical Trials Biospecimen Core Repository (BCR) • Tumor Pathology QC • % Tumor Nuclei • % Necrosis • Dx Confirmation via histology and pathology report • Molecular Analyte QC • Spectrophotometry • RNA Bioanalyzer • Electrophoresis • Genotyping TCGA-like Genome Characterization Pipeline Exome seq Whole genome seq RNA seq MicroRNA seq Affy 6.0 SNP DNA Methylation Genome Data Analysis Centers (GDACs) Genetic aberrations:Mutations Copy number Translocations Data analysis: GEP / miRNA / methylation subgroups Co-occurrence / exclusion Comparison to prior TCGA samples Data integration: Functional vs. structural Master regulator analysis Pathway analysis
Shifting the NCI Paradigm for Clinical Studies • Collect, store and annotate biospecimens from all/most patients on NCI clinical trials • FULL genomic characterization • Competition for pivotal trials with central funds • Encourage competition from grant pool • Incorporate essential epidemiological data Ex: ALChEMIST questionnaire
CCG Role in Precision Medicine • Enable NCI clinical trials to use genomic data optimally: • Understand response/resistance to Rx • Comparison of cases on different trials • Unify data and computational resources
Acknowledgements Kenna Liming Roy Zhining Emma Margi John Julia Martin Greg Pritty Shaw Yang Tarnuzzer Wang Spaulding Sheth Demchok Zhang Ferguson Eley Joshi
TCGA Program Office Responsibilities 25+ >500 1 3 Sequencing Centers Disease Working Groups Tissue Source Sites 5 Characterization Centers Biospecimen Core Resource 2 Data Portals • MTA/IRB review • Path review • Molecular co-isolation • Analyte QC including RIN • Door to door tracking of all samples • Collection of clinical data • Distribution of all molecular and clinical data to DCC • Coordination of expert pathology committees • MSI, SNP, HPV testing • Shipments to centers • MTA • IRB • Contract • Specimen Collection • Pre screening & path review • Deliver • Pathology Reports • Images • Clinical Data • Follow up • Inclusion specifications • CRFs • Identification of Tissue Source Sites • Often more than one group for each of the 25+ tumor projects 6 GDACs
Biospecimen Core Resource Review Whole Genome Amplification (Qiagen) BCR Characterization Centers Collection of Clinical Data Elements Tissue Source Sites (TSS) Preliminary Pathology Review Qualified • Tumor Pathology QC • % Tumor Nuclei • % Necrosis • Dx Confirmation via histology and pathology report Data Coordinating Center • Molecular Analyte QC • Spectrophotometery • RNA Bioanalyzer • Electrophoresis • Genotyping Sequencing Centers Diagram courtesy R. Penny, International Genomics Consortium
TCGA: Platforms- Then and Now *- Not a core platform; Not all samples will have data file for this platform More information on platforms and data available at: http:/tcga-data.nci.nih.gov/tcga/tcgaPlatformDesign.jsp
Minimum Clinical Data Set (100% required) • TSS name/identifier/patient # • Primary site of disease • Histological type • Tumor grade • Gender • Date of birth (month/year) • Prior diagnosis of prior neoplasm (if yes, another form required) • Date of initial pathologic diagnosis (month/year) • Neoadjuvant therapy • Tumor stage • Date of last contact (month/year) • Vital status (month/year) • Date of death, if applicable (month/year) • Tumor-type specific elements developed by Tumor Project Group
Examples of Tumor Specific Questions • Smoking status (lung/bladder) • ER/PR/Her2+ (breast) • Biochemical recurrence (prostate) • Residual tumor after surgery (ovarian/sarcoma) • Prior malignancy details (melanoma) • International Prognostic Index (lymphoma)
TCGA Data Portal https://tcga-data.nci.nih.gov/tcga/